PATH, Sexual & Reproductive Health Program, Seattle, USA.
Asociación Hondureña de Planificación de Familia, Tegucigalpa, Honduras.
Glob Health Sci Pract. 2020 Jun 30;8(2):290-299. doi: 10.9745/GHSP-D-19-00404.
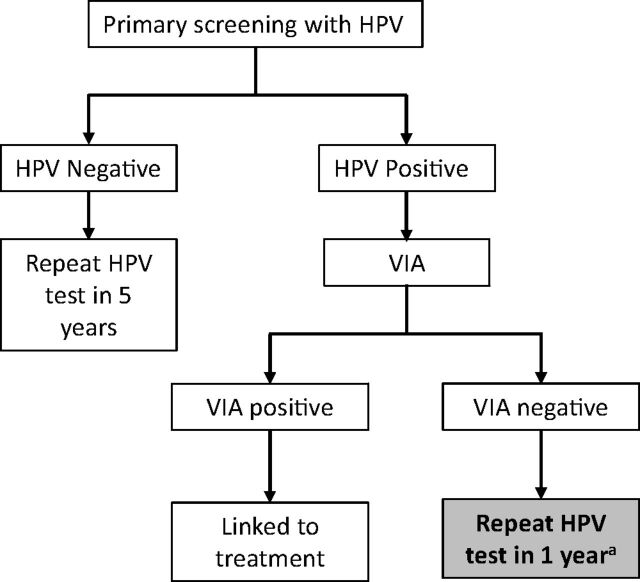
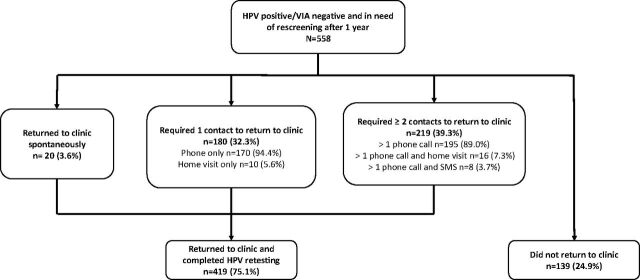
Scaling up coverage of routine cervical screening in low-resource settings must be accompanied by efforts to retain women throughout the screening cascade and continuum of care, including adequate follow-up of abnormal results. The Scale-Up Project implemented human papillomavirus (HPV) testing for cervical cancer screening within public-sector health facilities in Honduras between 2015 and 2019. Women who were HPV-positive but did not have visually confirmed cervical lesions upon visual inspection with acetic acid (VIA-negative) were instructed to return to the health center after 1 year for repeat HPV testing. The current evaluation assessed the effectiveness of recall strategies to prompt women to return for retesting. Clinic staff placed reminder phone calls and followed up with short message service (SMS) or home visits, if needed. We summarized number of contacts, type of contacts, and time elapsed until return to the clinic, and used log-binomial regression to identify factors associated with return to the clinic. We identified 558 women who were initially HPV-positive VIA-negative from 8 clinics as needing repeat HPV testing 1 year later. Mean age was 43.2 years. Nearly all women (98.6%) were successfully contacted and 75.1% completed repeat HPV testing. The majority of contacts (65.4%) were phone calls, and nearly half of women who returned to the clinic (42.9%) did so after 1 contact. Mean days between contact and presentation at the clinic was 10.7 (standard deviation: 14.7). Women who required 3 or more contacts were 21% less likely to return for repeat HPV testing (prevalence ratio: 0.79; 95% confidence interval=0.69,0.90; <.001) as compared to women who received only 1 contact. Reminder phone calls were highly successful at recalling women for HPV retesting in Honduras. This low-touch intervention should be included as part of standard follow-up to retain women throughout the continuum of cervical cancer screening and treatment.
在资源有限的环境中扩大常规宫颈筛查的覆盖范围,必须努力在整个筛查级联和护理连续体中留住女性,包括对异常结果进行充分的随访。2015 年至 2019 年,Scale-Up 项目在洪都拉斯的公立卫生机构中实施了人乳头瘤病毒(HPV)检测宫颈癌筛查。HPV 检测阳性但醋酸视觉检查(VIA 阴性)未见明显宫颈病变的女性,被指示在 1 年后返回卫生中心再次接受 HPV 检测。目前的评估评估了召回策略的有效性,以促使女性返回接受复查。诊所工作人员会打电话提醒,如有需要,还会通过短信服务(SMS)或家访进行跟进。我们总结了联系次数、联系类型以及到返回诊所的时间,并使用对数二项式回归来确定与返回诊所相关的因素。我们从 8 家诊所中确定了 558 名最初 HPV 阳性 VIA 阴性的女性,这些女性需要在 1 年后再次接受 HPV 检测。平均年龄为 43.2 岁。几乎所有女性(98.6%)都成功联系上,75.1%的女性完成了重复 HPV 检测。大多数联系(65.4%)是电话联系,返回诊所的女性中有近一半(42.9%)在 1 次联系后返回。从联系到在诊所就诊的平均天数为 10.7 天(标准差:14.7)。需要 3 次或更多联系的女性再次接受 HPV 检测的可能性降低 21%(流行率比:0.79;95%置信区间=0.69,0.90;<0.001),而仅接受 1 次联系的女性则没有。提醒电话在召回女性进行 HPV 复查方面非常成功。在洪都拉斯,这种低接触干预措施应该作为标准随访的一部分,以在整个宫颈癌筛查和治疗连续体中留住女性。