Vardarli Irfan, Rischpler Christoph, Herrmann Ken, Weidemann Frank
Department of Medicine I, Klinikum Vest, Knappschaftskrankenhaus Recklinghausen, Academic Teaching Hospital, Ruhr-University Bochum, Recklinghausen, Germany.
Herz- Und Gefäßzentrum Klinikum Vest, Recklinghausen, Germany.
Ther Clin Risk Manag. 2020 Jun 22;16:551-558. doi: 10.2147/TCRM.S247814. eCollection 2020.
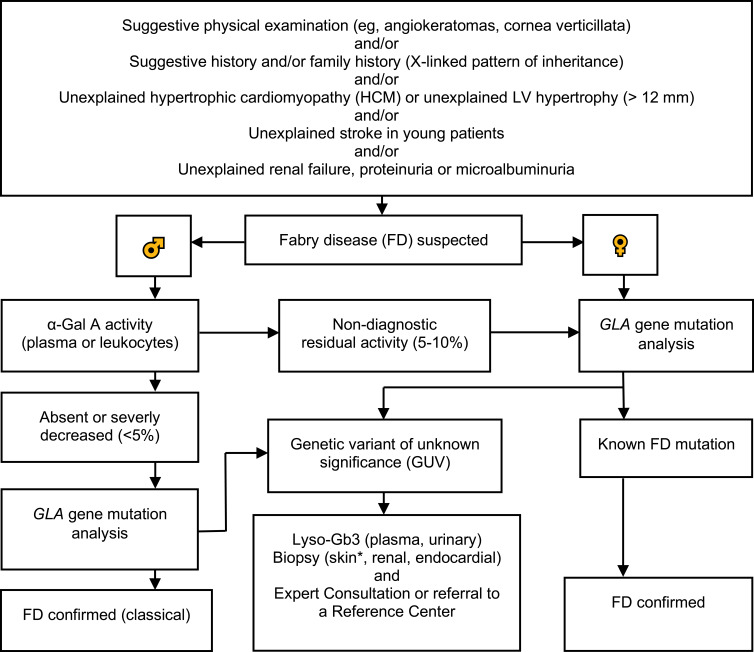
Fabry disease (FD) is an X-linked lysosomal storage disorder caused by absence or deficient activity of α-galactosidase A (α-Gal A) due to mutations in the α-galactosidase A gene (), leading to progressive accumulation of globotriaosylceramide (Gb3) in tissues and organs including heart, kidney, the eyes, vascular endothelium, the nervous system and the skin. Cardiac involvement is leading to fatal complications and reduced life expectancy. FD is treatable with disease-specific treatment (enzyme replacement therapy (ERT) or with chaperone therapy). Therefore, the early diagnosis of FD is crucial for reducing the morbidity and mortality. Screening of high-risk populations (eg, patients with unexplained left ventricular hypertrophy (LVH), young patients with unexplained stroke, and patients with unexplained renal failure proteinuria or microalbuminuria) yields good results. The diagnostic algorithm is gender-specific. Initially, the measurement of α-Gal A activity is recommended in males, and optionally in females. In males with non-diagnostic residual activity (5-10%) activity, genetic testing is afterwards done for confirming the diagnosis. In fact, diagnosis of FD is not possible without genetic testing for both males and females. Globotriaosysphingosine (lyso-Gb3) for identification of atypical FD variants and high- sensitive troponin T (hsTNT) for identification of cardiac involvement are also important diagnostic biomarkers. The aim of this review was to provide an update on diagnosis and screening of patients with FD.
法布里病(FD)是一种X连锁溶酶体贮积症,由α-半乳糖苷酶A(α-Gal A)基因()突变导致α-半乳糖苷酶A缺乏或活性不足引起,导致球三糖神经酰胺(Gb3)在心脏、肾脏、眼睛、血管内皮、神经系统和皮肤等组织和器官中进行性蓄积。心脏受累会导致致命并发症并缩短预期寿命。FD可通过疾病特异性治疗(酶替代疗法(ERT)或伴侣疗法)进行治疗。因此,FD的早期诊断对于降低发病率和死亡率至关重要。对高危人群(如原因不明的左心室肥厚(LVH)患者、原因不明的中风年轻患者以及原因不明的肾衰竭蛋白尿或微量白蛋白尿患者)进行筛查可取得良好效果。诊断算法具有性别特异性。最初,建议对男性进行α-Gal A活性检测,女性可选择检测。对于残余活性为非诊断性(5-10%)的男性,随后进行基因检测以确诊。事实上,无论男性还是女性,不进行基因检测都无法诊断FD。用于识别非典型FD变体的球三糖鞘氨醇(lyso-Gb3)和用于识别心脏受累的高敏肌钙蛋白T(hsTNT)也是重要的诊断生物标志物。本综述的目的是提供FD患者诊断和筛查的最新情况。