Department of Medicine, University of Vermont, Burlington, Vermont, USA.
Department of Orthopaedics and Rehabilitation, University of Vermont, Burlington, Vermont, USA.
Am J Sports Med. 2020 Aug;48(10):2429-2437. doi: 10.1177/0363546520933622. Epub 2020 Jul 6.
Anterior cruciate ligament (ACL) injuries and reconstruction (ACLR) promote quadriceps muscle atrophy and weakness that can persist for years, suggesting the need for more effective rehabilitation programs. Whether neuromuscular electrical stimulation (NMES) can be used to prevent maladaptations in skeletal muscle size and function is unclear.
To examine whether early NMES use, started soon after an injury and maintained through 3 weeks after surgery, can preserve quadriceps muscle size and contractile function at the cellular (ie, fiber) level in the injured versus noninjured leg of patients undergoing ACLR.
Randomized controlled trial; Level of evidence, 1.
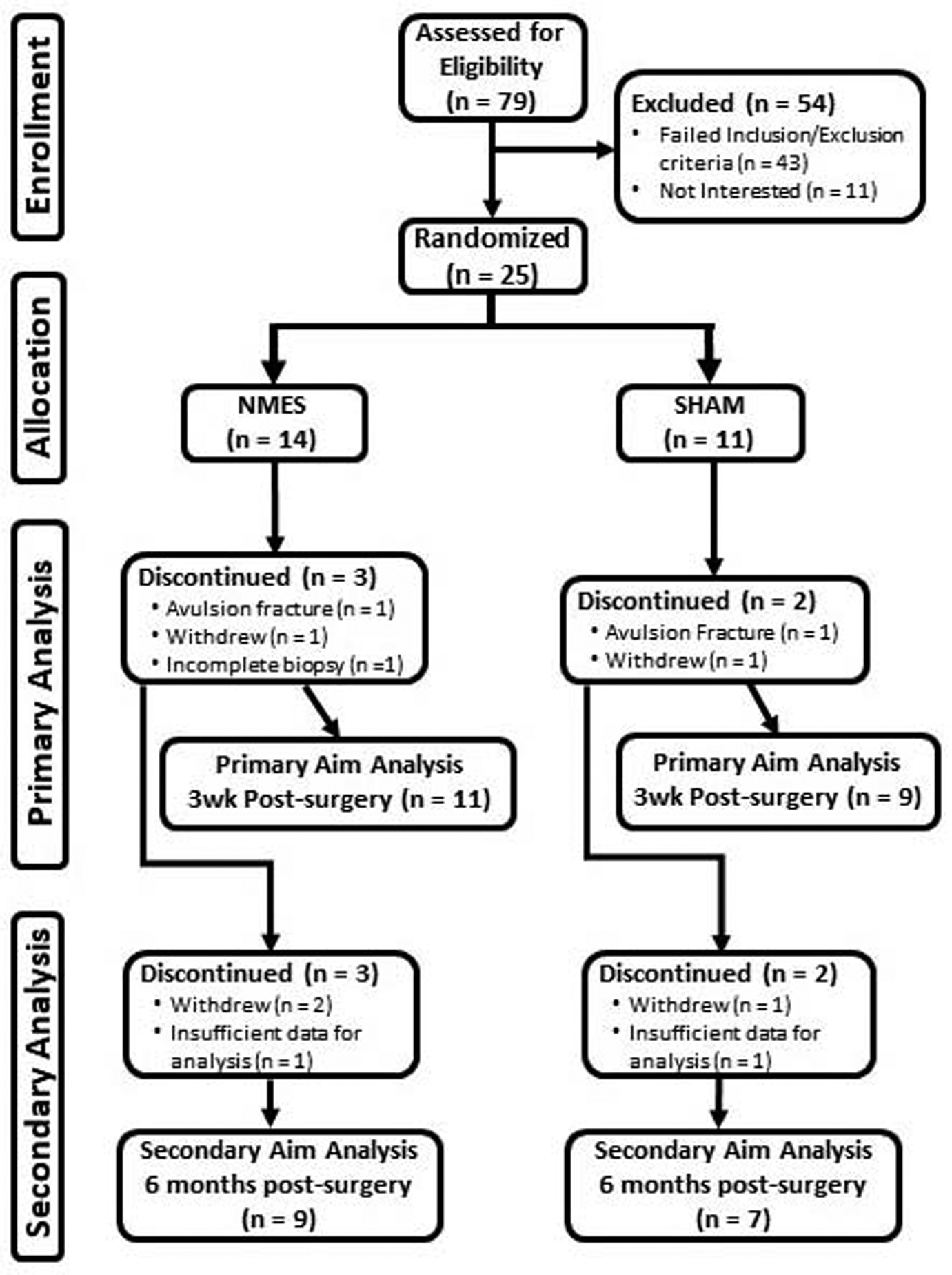
Patients (n = 25; 12 men/13 women) with an acute, first-time ACL rupture were randomized to NMES (5 d/wk) or sham (simulated microcurrent electrical nerve stimulation; 5 d/wk) treatment to the quadriceps muscles of their injured leg. Bilateral biopsies of the vastus lateralis were performed 3 weeks after surgery to measure skeletal muscle fiber size and contractility. Quadriceps muscle size and strength were assessed 6 months after surgery.
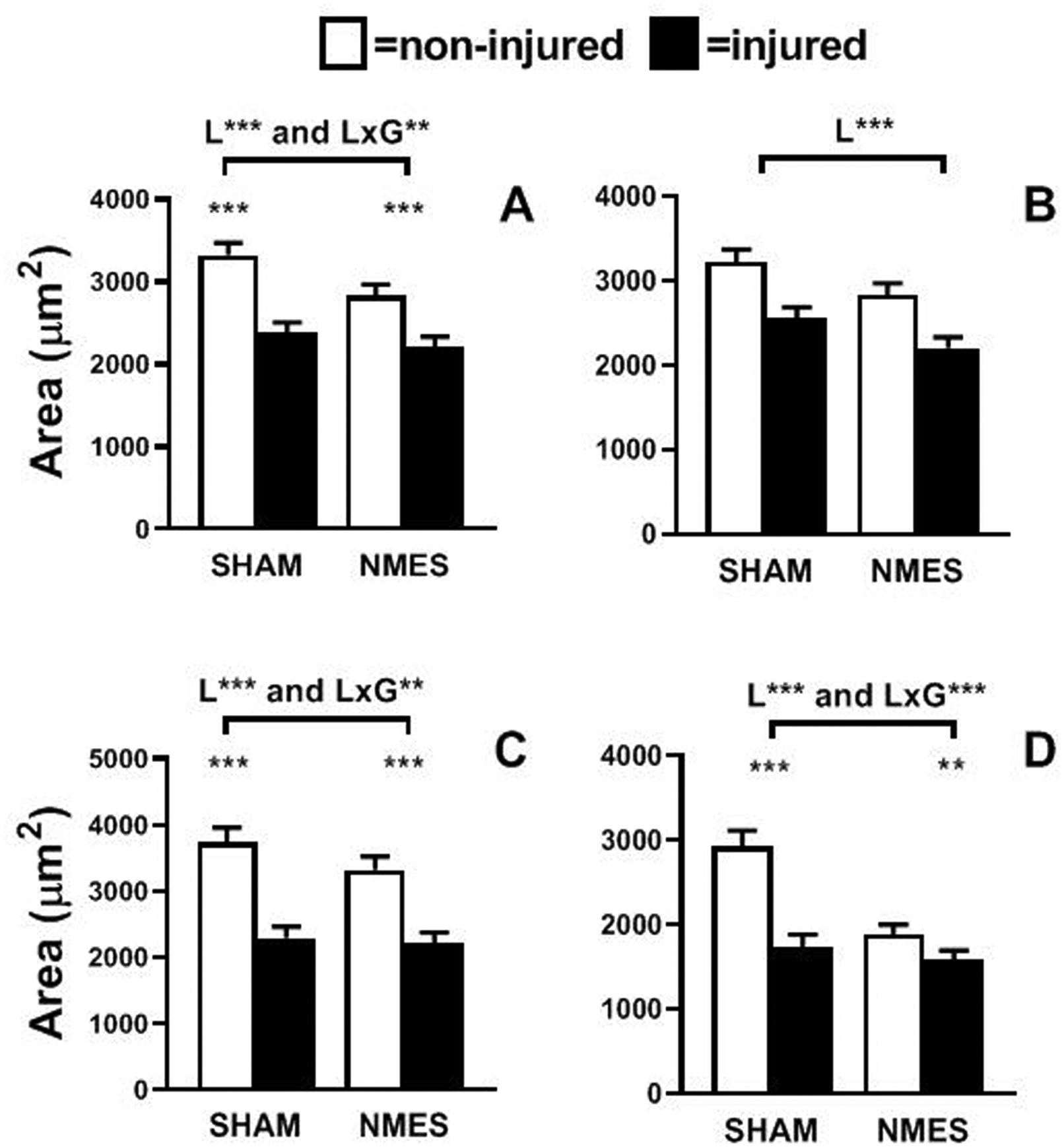
A total of 21 patients (9 men/12 women) completed the trial. ACLR reduced single muscle fiber size and contractility across all fiber types ( < .01 to < .001) in the injured compared with noninjured leg 3 weeks after surgery. NMES reduced muscle fiber atrophy ( < .01) through effects on fast-twitch myosin heavy chain (MHC) II fibers ( < .01 to < .001). NMES preserved contractility in slow-twitch MHC I fibers ( < .01 to < .001), increasing maximal contractile velocity ( < .01) and preserving power output ( < .01), but not in MHC II fibers. Differences in whole muscle strength between groups were not discerned 6 months after surgery.
Early NMES use reduced skeletal muscle fiber atrophy in MHC II fibers and preserved contractility in MHC I fibers. These results provide seminal, cellular-level data demonstrating the utility of the early use of NMES to beneficially modify skeletal muscle maladaptations to ACLR.
Our results provide the first comprehensive, cellular-level evidence to show that the early use of NMES mitigates early skeletal muscle maladaptations to ACLR.
NCT02945553 (ClinicalTrials.gov identifier).
前交叉韧带(ACL)损伤和重建(ACLR)会导致股四头肌萎缩和无力,这种情况可能会持续数年,这表明需要更有效的康复方案。神经肌肉电刺激(NMES)是否可以用于防止骨骼肌肉大小和功能的适应不良尚不清楚。
研究在 ACLR 患者受伤腿的 NMES 是否可以在细胞(即纤维)水平上预防股四头肌肌肉大小和收缩功能的损伤和非损伤侧的适应不良。
随机对照试验;证据水平,1 级。
将 25 名(12 名男性/13 名女性)急性初次 ACL 撕裂的患者随机分为 NMES(每周 5 天)或假(模拟微电流神经刺激;每周 5 天)治疗组,以治疗受伤腿的股四头肌。在手术后 3 周对股外侧肌进行双侧活检,以测量骨骼肌纤维大小和收缩性。手术后 6 个月评估股四头肌大小和力量。
共有 21 名患者(9 名男性/12 名女性)完成了试验。ACL 重建后 3 周,受伤腿的单个肌纤维大小和收缩性在所有纤维类型中均降低(<.01 至<.001)。NMES 通过对快肌肌球蛋白重链(MHC)II 纤维的作用减少了肌肉纤维萎缩(<.01)(<.01 至<.001)。NMES 保留了慢肌 MHC I 纤维的收缩性(<.01 至<.001),增加了最大收缩速度(<.01)并保留了功率输出(<.01),但对 MHC II 纤维则不然。手术后 6 个月,两组之间的整体肌肉力量差异并不明显。
早期 NMES 使用减少了 MHC II 纤维中的骨骼肌纤维萎缩,并保留了 MHC I 纤维的收缩性。这些结果提供了开创性的细胞水平数据,证明了早期使用 NMES 有益地改变 ACLR 后骨骼肌肉的适应不良。
我们的结果提供了第一个全面的细胞水平证据,表明早期使用 NMES 可以减轻 ACLR 对早期骨骼肌的适应不良。
NCT02945553(ClinicalTrials.gov 标识符)。