Department of Physiology, Research Institute for Health Sciences, Radboud University Medical Center, Philips van Leijdenlaan 15, 6525 EX Nijmegen, The Netherlands.
Department of Cardiology, Research Institute for Health Sciences, Radboud University Medical Center, Geert Grooteplein Zuid 10 6525 GA Nijmegen, The Netherlands.
Eur Heart J Cardiovasc Imaging. 2021 Jan 22;22(2):188-195. doi: 10.1093/ehjci/jeaa143.
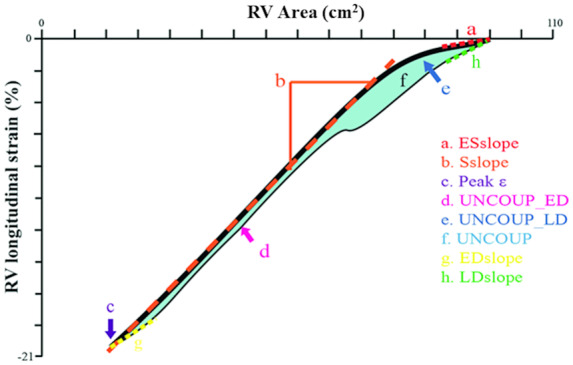
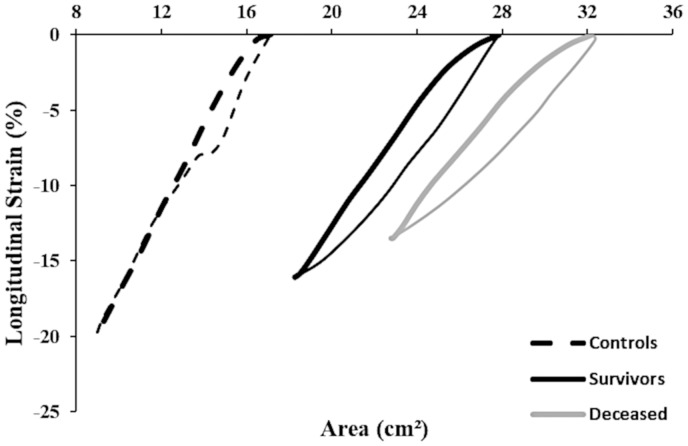
Patients with pre-capillary pulmonary hypertension (PH) show poor survival, often related to right ventricular (RV) dysfunction. In this study, we assessed the 5-year prognostic value of a novel echocardiographic measure that examines RV function through the temporal relation between RV strain (ϵ) and area (i.e. RV ϵ-area loop) for all-cause mortality in PH patients.
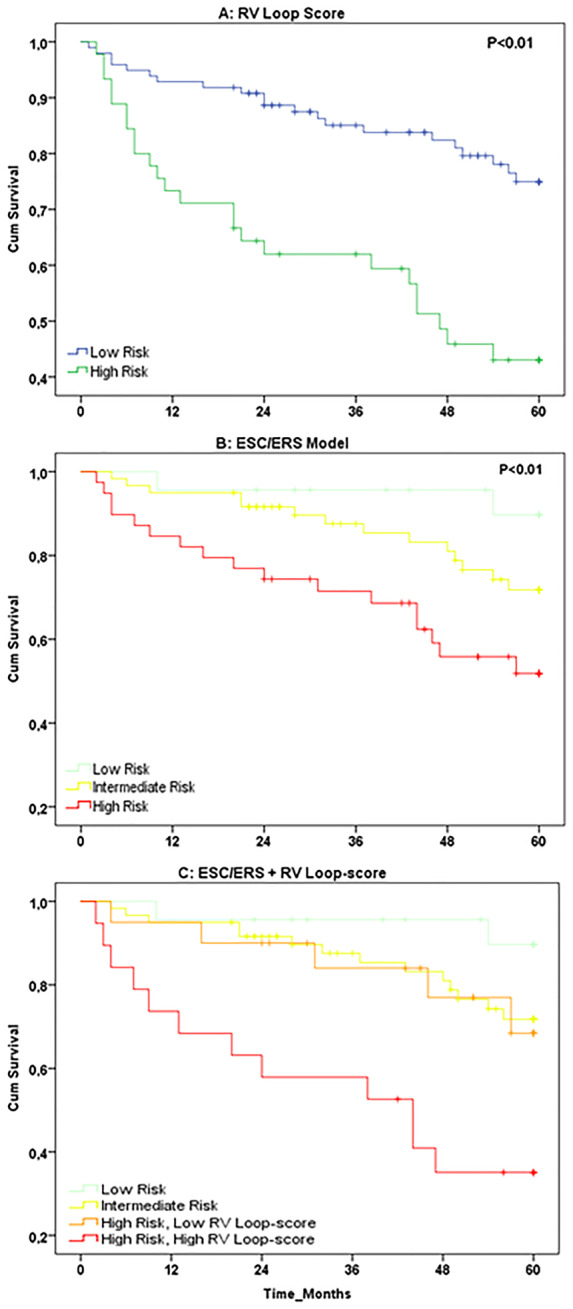
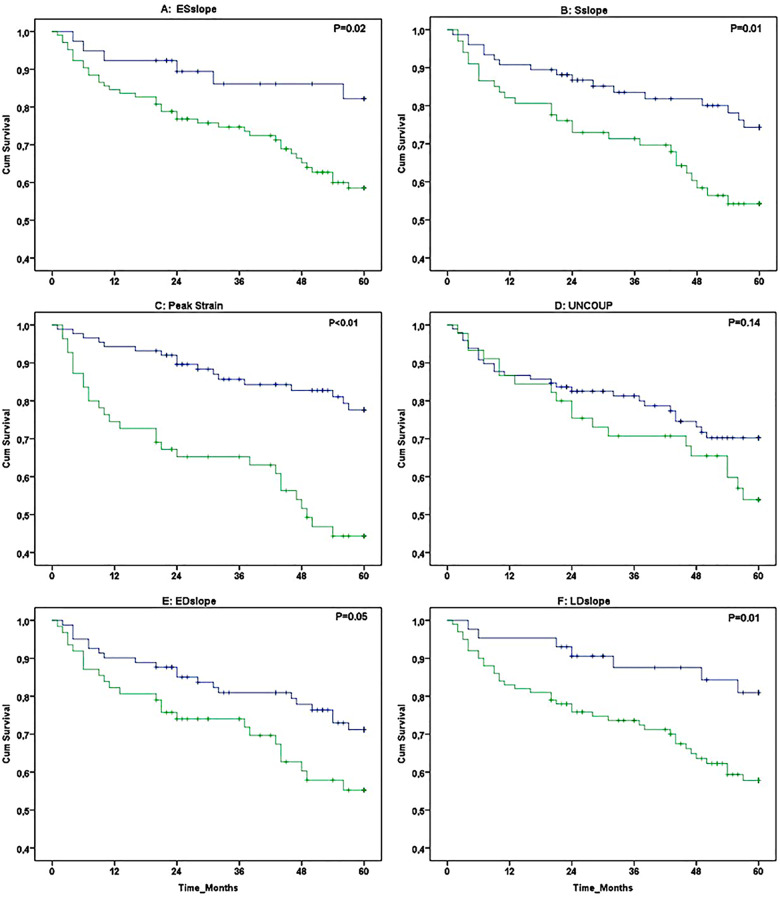
Echocardiographic assessments were performed in 143 PH patients (confirmed by right heart catheterization). Transthoracic echocardiography was utilized to assess RV ϵ-area loop. Using receiver operating characteristic curve-derived cut-off values, we stratified patients in low- vs. high-risk groups for all-cause mortality. Kaplan-Meier survival curves and uni-/multivariable cox-regression models were used to assess RV ϵ-area loop's prognostic value (independent of established predictors: age, sex, N-terminal pro B-type natriuretic peptide, 6-min walking distance). During follow-up 45 (31%) patients died, who demonstrated lower systolic slope, peak ϵ, and late diastolic slope (all P < 0.05) at baseline. Univariate cox-regression analyses identified early systolic slope, systolic slope, peak ϵ, early diastolic uncoupling, and early/late diastolic slope to predict all-cause mortality (all P < 0.05), whilst peak ϵ possessed independent prognostic value (P < 0.05). High RV loop-score (i.e. based on number of abnormal characteristics) showed poorer survival compared to low RV loop-score (Kaplan-Meier: P < 0.01). RV loop-score improved risk stratification in high-risk patients when added to established predictors.
Our data demonstrate the potential for RV ϵ-area loops to independently predict all-cause mortality in patients with pre-capillary PH. The non-invasive nature and simplicity of measuring the RV ϵ-area loop, support the potential clinical relevance of (repeated) echocardiography assessment of PH patients.
患有毛细血管前肺高血压(PH)的患者生存率较差,这通常与右心室(RV)功能障碍有关。在这项研究中,我们评估了一种新的超声心动图指标的 5 年预后价值,该指标通过 RV 应变(ϵ)与面积之间的时间关系(即 RV ϵ-面积环)来评估 PH 患者的全因死亡率。
对 143 例 PH 患者(通过右心导管检查确诊)进行了超声心动图评估。经胸超声心动图用于评估 RV ϵ-面积环。使用接受者操作特征曲线得出的截断值,我们将患者分为低危和高危全因死亡率组。使用 Kaplan-Meier 生存曲线和单变量/多变量 Cox 回归模型评估 RV ϵ-面积环的预后价值(独立于既定预测因子:年龄、性别、N 末端 B 型利钠肽前体、6 分钟步行距离)。在随访期间,有 45 名(31%)患者死亡,他们在基线时表现出较低的收缩斜率、峰值 ϵ 和舒张晚期斜率(均 P<0.05)。单变量 Cox 回归分析确定了早期收缩斜率、收缩斜率、峰值 ϵ、早期舒张去耦和早期/晚期舒张斜率来预测全因死亡率(均 P<0.05),而峰值 ϵ 具有独立的预后价值(P<0.05)。高 RV 环评分(即基于异常特征的数量)与低 RV 环评分相比,生存率较差(Kaplan-Meier:P<0.01)。当 RV 环评分添加到既定预测因子中时,可改善高危患者的风险分层。
我们的数据表明,RV ϵ-面积环可独立预测毛细血管前 PH 患者的全因死亡率。RV ϵ-面积环的非侵入性和测量的简单性支持对 PH 患者进行(重复)超声心动图评估的潜在临床相关性。