Vallabhajosyula Saraschandra, Dunlay Shannon M, Bell Malcolm R, Miller P Elliott, Cheungpasitporn Wisit, Sundaragiri Pranathi R, Kashani Kianoush, Gersh Bernard J, Jaffe Allan S, Holmes David R, Barsness Gregory W
Department of Cardiovascular Medicine, Mayo Clinic, Rochester, MN 55905, USA.
Division of Pulmonary and Critical Care Medicine, Department of Medicine, Mayo Clinic, Rochester, MN 55905, USA.
J Clin Med. 2020 Jul 3;9(7):2094. doi: 10.3390/jcm9072094.
There are limited data on the epidemiology and timing of in-hospital death (IHD) in patients with acute myocardial infarction-cardiogenic shock (AMI-CS).
Adult admissions with AMI-CS with IHDs were identified using the National Inpatient Sample (2000-2016) and were classified as early (≤2 days), mid-term (3-7 days), and late (>7 days). Inter-hospital transfers and those with do-not-resuscitate statuses were excluded. The outcomes of interest included the epidemiology, temporal trends and predictors for IHD timing.
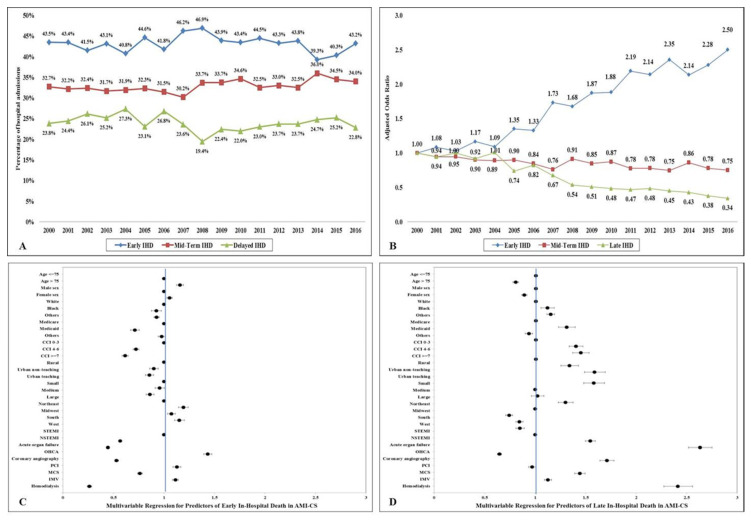
IHD was noted in 113,349 AMI-CS admissions (median time to IHD 3 (interquartile range 1-7) days), with early, mid-term and late IHD in 44%, 32% and 24%, respectively. Compared to the mid-term and late groups, the early IHD group had higher rates of ST-segment-elevation AMI-CS (74%, 63%, 60%) and cardiac arrest (37%, 33%, 29%), but lower rates of acute organ failure (68%, 79%, 89%), use of coronary angiography (45%, 56%, 67%), percutaneous coronary intervention (33%, 36%, 42%), and mechanical circulatory support (31%, 39%, 50%) (all < 0.001). There was a temporal increase in the early (adjusted odds ratio (aOR) for 2016 vs. 2000 2.50 (95% confidence interval (CI) 2.22-2.78)) and a decrease in mid-term (aOR 0.75 (95% CI 0.71-0.79)) and late (aOR 0.34 (95% CI 0.31-0.37)) IHD. ST-segment-elevation AMI-CS and cardiac arrest were associated with the increased risk of early IHD, whereas advanced comorbidity and acute organ failure were associated with late IHD.
Early IHD after AMI-CS has increased between 2000 and 2016. The populations with early vs. late IHD were systematically different.
关于急性心肌梗死合并心源性休克(AMI-CS)患者的院内死亡(IHD)流行病学及时间规律的数据有限。
利用国家住院患者样本(2000 - 2016年)确定患有AMI-CS且发生IHD的成年住院患者,并分为早期(≤2天)、中期(3 - 7天)和晚期(>7天)。排除院间转运患者及有“不要复苏”状态的患者。感兴趣的结局包括IHD的流行病学、时间趋势及IHD时间的预测因素。
在113,349例AMI-CS住院患者中发现了IHD(至IHD的中位时间为3天(四分位间距1 - 7天)),早期、中期和晚期IHD分别占44%、32%和24%。与中期和晚期组相比,早期IHD组ST段抬高型AMI-CS的发生率更高(分别为74%、63%、60%)以及心脏骤停发生率更高(分别为37%、33%、29%),但急性器官衰竭发生率更低(分别为68%、79%、89%),冠状动脉造影使用率更低(分别为45%、56%、67%),经皮冠状动脉介入治疗率更低(分别为33%、36%、42%)以及机械循环支持使用率更低(分别为31%、39%、50%)(均P<0.001)。早期IHD呈时间上的增加趋势(2016年与2000年相比,校正比值比(aOR)为2.50(95%置信区间(CI)2.22 - 2.78)),中期(aOR 0.75(95%CI 0.71 - 0.79))和晚期(aOR 0.34(95%CI 0.31 - 0.37))IHD呈下降趋势。ST段抬高型AMI-CS和心脏骤停与早期IHD风险增加相关,而晚期合并症和急性器官衰竭与晚期IHD相关。
2000年至2016年间,AMI-CS后的早期IHD有所增加。早期与晚期IHD的人群存在系统性差异。