Department of Cardiovascular Medicine, Mayo Clinic, Rochester, Minnesota, United states of America.
Division of Pulmonary and Critical Care Medicine, Department of Medicine, Mayo Clinic, Rochester, Minnesota, United states of America.
PLoS One. 2019 Sep 18;14(9):e0222894. doi: 10.1371/journal.pone.0222894. eCollection 2019.
There are limited data on acute kidney injury (AKI) complicating acute myocardial infarction with cardiogenic shock (AMI-CS). This study sought to evaluate 15-year national prevalence, temporal trends and outcomes of AKI with no need for hemodialysis (AKI-ND) and requiring hemodialysis (AKI-D) following AMI-CS.
This was a retrospective cohort study from 2000-2014 from the National Inpatient Sample (20% stratified sample of all community hospitals in the United States). Adult patients (>18 years) admitted with a primary diagnosis of AMI and secondary diagnosis of CS were included. The primary outcome was in-hospital mortality in cohorts with no AKI, AKI-ND, and AKI-D. Secondary outcomes included predictors, resource utilization and disposition.
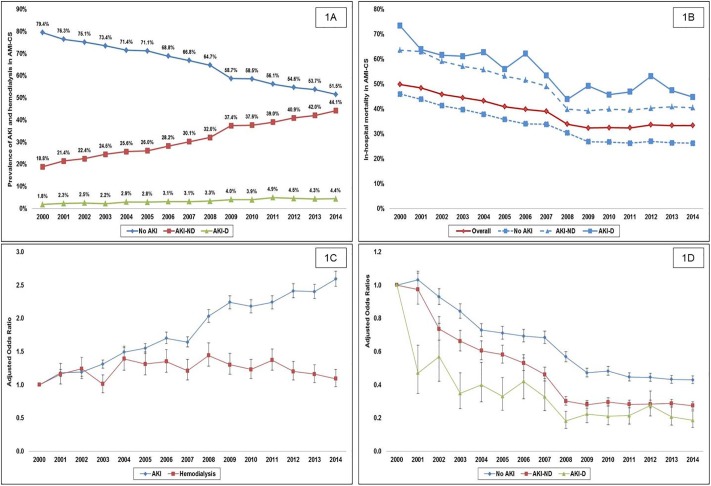
During this 15-year period, 440,257 admissions for AMI-CS were included, with AKI in 155,610 (35.3%) and hemodialysis use in 14,950 (3.4%). Older age, black race, non-private insurance, higher comorbidity, organ failure, and use of cardiac and non-cardiac organ support were associated with the AKI development and hemodialysis use. There was a 2.6-fold higher adjusted risk of developing AKI in 2014 compared to 2000. Presence of AKI-ND and AKI-D was associated with a 1.3 and 1.7-fold higher adjusted risk of mortality. Compared to the cohort without AKI, AKI-ND and AKI-D were associated with longer length of stay (9±10, 12±13, and 18±19 days respectively; p<0.001) and higher hospitalization costs ($101,859±116,204, $159,804±190,766, and $265,875 ± 254,919 respectively; p<0.001).
AKI-ND and AKI-D are associated with higher in-hospital mortality and resource utilization in AMI-CS.
关于伴心源性休克的急性心肌梗死(AMI-CS)并发急性肾损伤(AKI)的数据有限。本研究旨在评估 15 年来伴心源性休克的急性心肌梗死并发无需透析(AKI-ND)和需要透析(AKI-D)的 AKI 的全国患病率、时间趋势和结局。
这是一项回顾性队列研究,来自 2000 年至 2014 年的全国住院患者样本(美国所有社区医院的 20%分层样本)。纳入的成年患者(>18 岁)入院时的主要诊断为 AMI,次要诊断为 CS。主要结局为无 AKI、AKI-ND 和 AKI-D 患者的院内死亡率。次要结局包括预测因素、资源利用和处置。
在这 15 年期间,共纳入 440257 例 AMI-CS 入院患者,其中 AKI 患者 155610 例(35.3%),使用血液透析患者 14950 例(3.4%)。年龄较大、黑人、非私人保险、更高的合并症、器官衰竭以及使用心脏和非心脏器官支持与 AKI 发展和血液透析使用相关。与 2000 年相比,2014 年 AKI 发展的调整风险增加了 2.6 倍。存在 AKI-ND 和 AKI-D 与调整后死亡率增加 1.3 倍和 1.7 倍相关。与无 AKI 的患者相比,AKI-ND 和 AKI-D 患者的住院时间更长(分别为 9±10、12±13 和 18±19 天;p<0.001),住院费用更高(分别为 101859±116204、159804±190766 和 265875±254919;p<0.001)。
伴心源性休克的急性心肌梗死并发 AKI-ND 和 AKI-D 与更高的院内死亡率和资源利用相关。