Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea.
Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea.
J Cachexia Sarcopenia Muscle. 2020 Oct;11(5):1232-1241. doi: 10.1002/jcsm.12598. Epub 2020 Jul 7.
We investigated the association between muscle strength and the prevalence of advanced fibrosis among individuals with non-alcoholic fatty liver disease (NAFLD) using a nationwide cross-sectional survey.
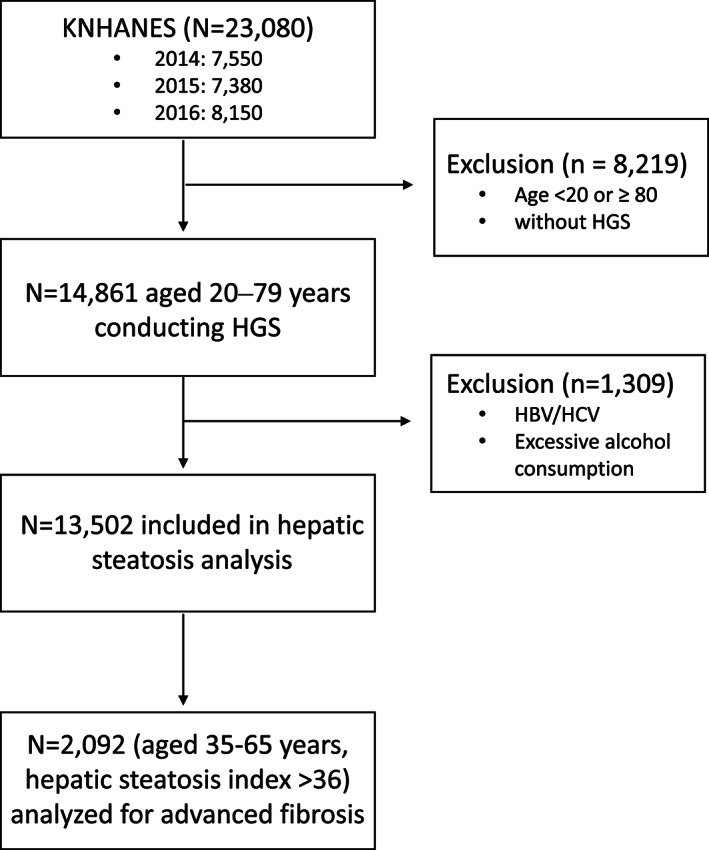
Individuals, 20 to 79 years of age, from the Korean National Health and Nutrition Examination Surveys (KNHANES) from 2014 to 2016 were selected (N = 14 861), with sample weights applied. Muscle strength was quantified as the handgrip strength divided by the body mass index (BMI); low muscle strength (LMS) was defined as the lowest quartile (Q ) of the handgrip strength/BMI for our sample population. NAFLD was defined as hepatic steatosis index >36. Advanced fibrosis was defined as a fibrosis-4 index score ≥1.30 (Fibrosis ).
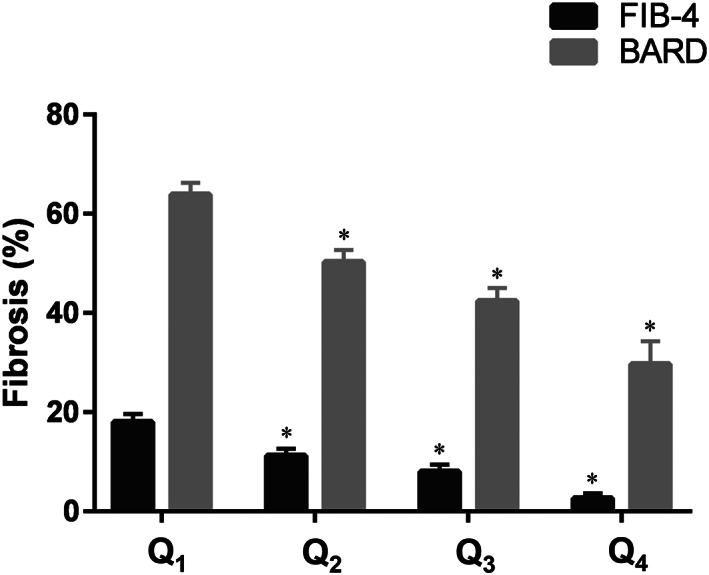
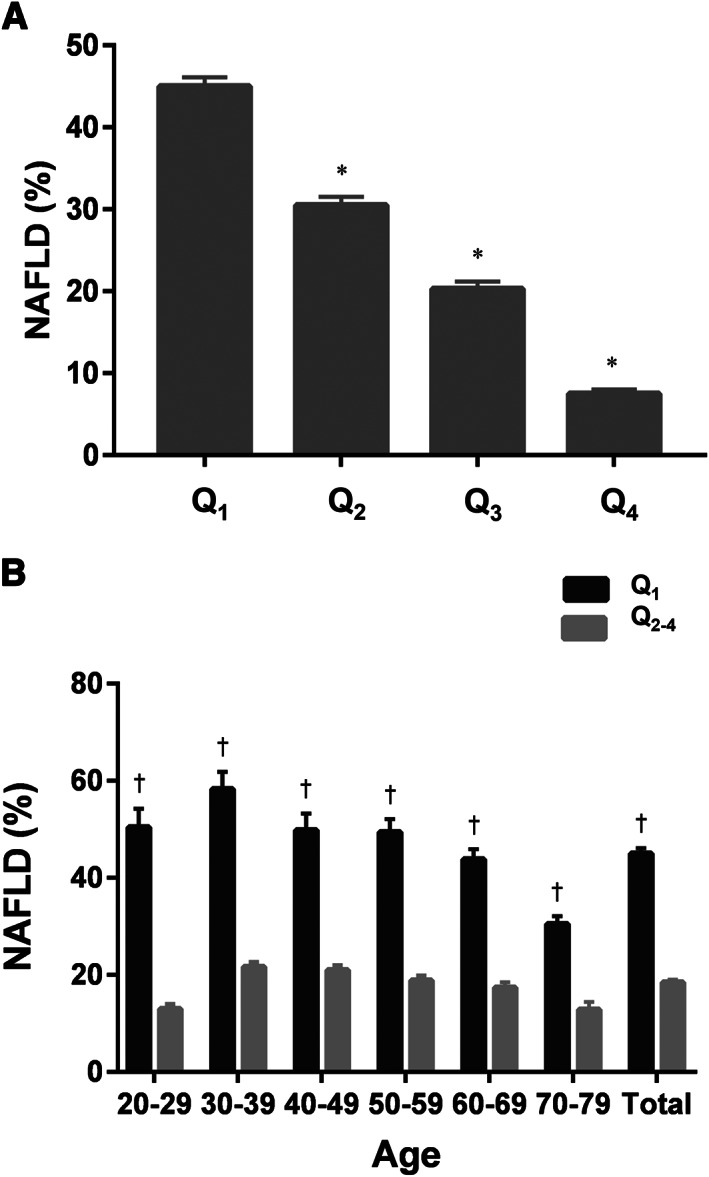
The mean age of the study population was 45.6 ± 0.2 years, and 42.4% were male. As muscle strength increased, the mean BMI and age decreased accordingly, and the proportions of diabetes, dyslipidaemia, hypertension, and obesity decreased significantly (P < 0.001 for all). In a crude analysis, the LMS was associated with an increased prevalence of NAFLD (odds ratio [OR] 3.62, 95% confidence interval [CI] 3.25-4.03, P < 0.001), which remained significant even after adjustment for age, sex, obesity, insulin resistance, diabetes, hypertension, dyslipidaemia, and high-sensitivity C-reactive protein (OR 1.66, 95% CI 1.28-2.16, P < 0.001). In this logistic regression model, the prevalence of NAFLD decreased by 24% with each quartile increment in muscle strength (OR 0.76, 95% CI 0.68-0.85, P < 0.001). Among individuals with NAFLD (n = 2092), LMS was significantly associated with the presence of advanced fibrosis (Fibrosis ) independently of age, sex, obesity, diabetes, hypertension, dyslipidaemia, and high-sensitivity C-reactive protein (OR 1.66, 95% CI 1.01-2.49, P = 0.015), which lost its statistical significance after additional adjustment for insulin resistance.
Low muscle strength is independently associated with NAFLD. The significant association between LMS and advanced fibrosis in NAFLD may be mediated through insulin resistance.
我们通过全国性横断面调查研究了非酒精性脂肪性肝病(NAFLD)患者肌肉力量与晚期纤维化患病率之间的关系。
我们从 2014 年至 2016 年的韩国国家健康和营养检查调查(KNHANES)中选择了 20 至 79 岁的个体(N=14861),并应用了样本权重。肌肉力量用握力除以体重指数(BMI)来量化;低肌肉力量(LMS)定义为我们样本人群中握力/BMI 的最低四分位数(Q)。NAFLD 定义为肝脂肪指数>36。晚期纤维化定义为纤维化-4 指数评分≥1.30(Fibrosis)。
研究人群的平均年龄为 45.6±0.2 岁,其中 42.4%为男性。随着肌肉力量的增加,平均 BMI 和年龄相应下降,糖尿病、血脂异常、高血压和肥胖的比例显著降低(所有 P<0.001)。在未调整分析中,LMS 与 NAFLD 的患病率增加相关(比值比[OR]3.62,95%置信区间[CI]3.25-4.03,P<0.001),即使在调整年龄、性别、肥胖、胰岛素抵抗、糖尿病、高血压、血脂异常和高敏 C 反应蛋白(hs-CRP)后仍有显著意义(OR 1.66,95%CI 1.28-2.16,P<0.001)。在这个逻辑回归模型中,肌肉力量每增加一个四分位,NAFLD 的患病率就会降低 24%(OR 0.76,95%CI 0.68-0.85,P<0.001)。在患有 NAFLD 的个体(n=2092)中,LMS 与晚期纤维化(Fibrosis)的存在显著相关,独立于年龄、性别、肥胖、糖尿病、高血压、血脂异常和 hs-CRP(OR 1.66,95%CI 1.01-2.49,P=0.015),但在进一步调整胰岛素抵抗后,其统计学意义丧失。
低肌肉力量与 NAFLD 独立相关。LMS 与 NAFLD 晚期纤维化之间的显著关联可能通过胰岛素抵抗介导。