Department of Pathology, School of Medicine, Johns Hopkins University, Baltimore, Maryland.
Department of Epidemiology, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Maryland.
Prostate. 2020 Sep;80(12):1012-1023. doi: 10.1002/pros.24035. Epub 2020 Jul 10.
Small cell neuroendocrine (NE) carcinomas of the prostate classically lose androgen receptor (AR) expression, may harbor loss of the RB1, TP53, and PTEN tumor suppressor genes, and are associated with a poor prognosis. However usual-type adenocarcinomas may also contain areas of NE differentiation, and in this context the molecular features and biological significance are less certain.
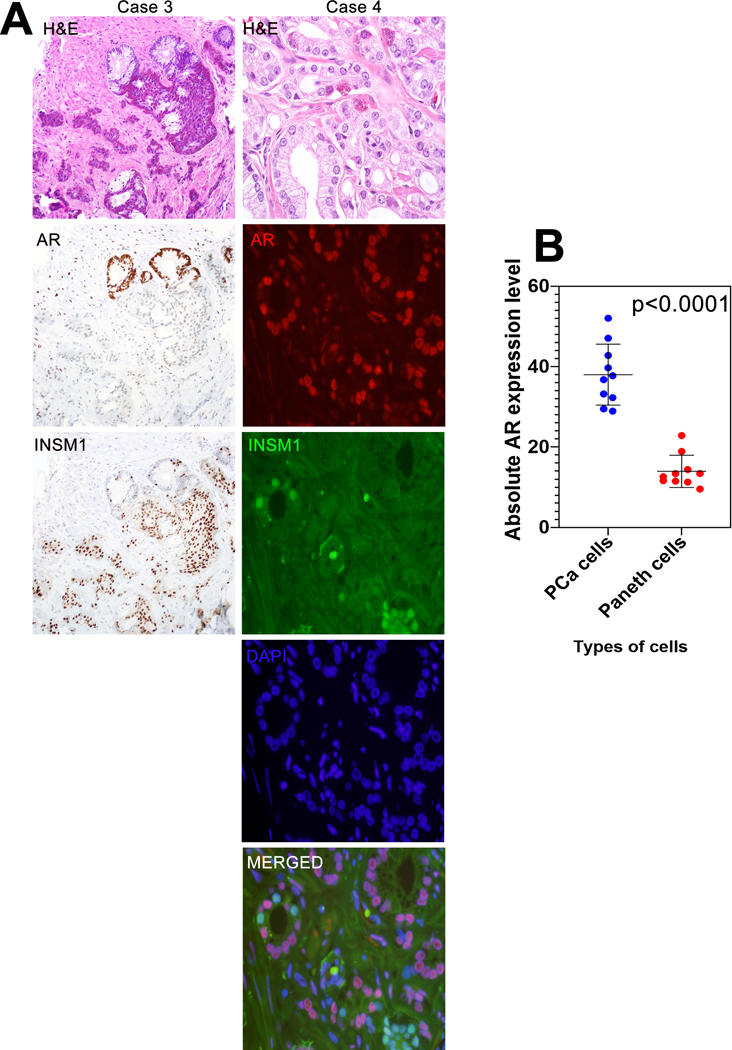
We examined the molecular phenotype and oncologic outcomes of primary prostate adenocarcinomas with ≥5% NE differentiation (≥5% chromogranin A-positive NE cells in any given tumor spot on tissue microarray) using three independent study sets: a set of tumors with paneth cell-like NE differentiation (n = 26), a retrospective case-cohort of intermediate- and high-risk patients enriched for adverse outcomes (n = 267), and primary tumors from a retrospective series of men with eventual castration-resistant metastatic prostate cancer (CRPC) treated with abiraterone or enzalutamide (n = 55).
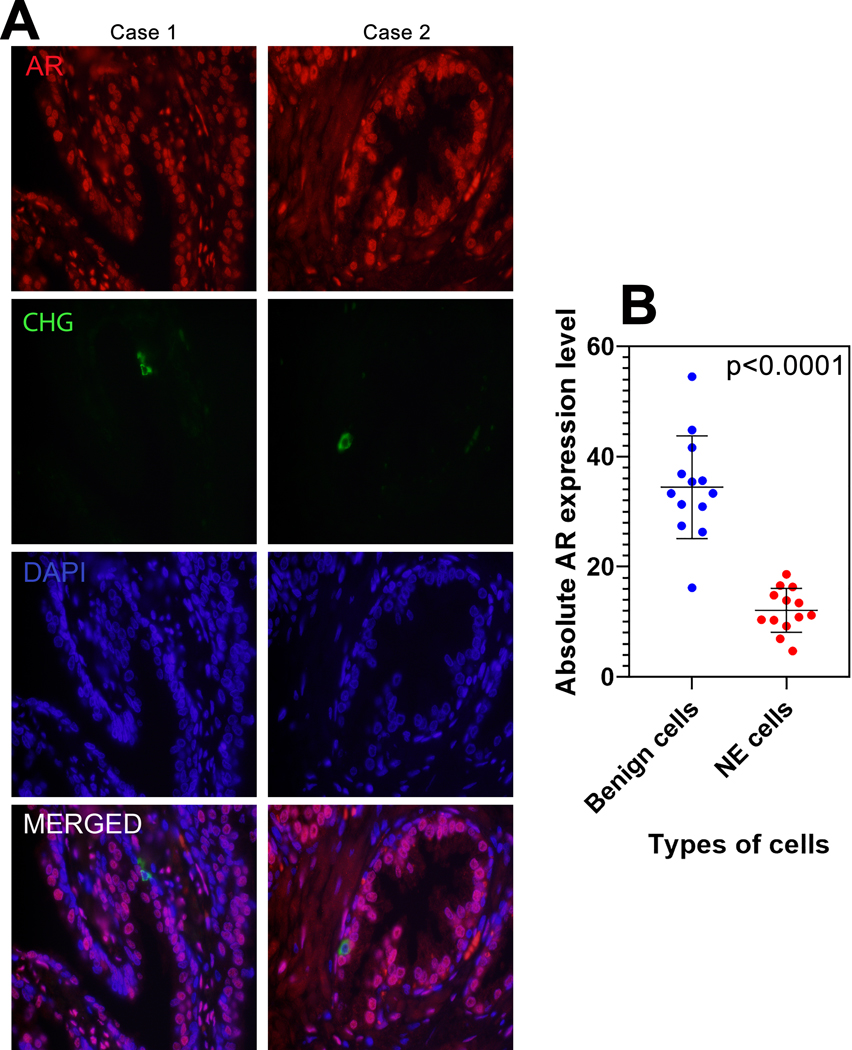
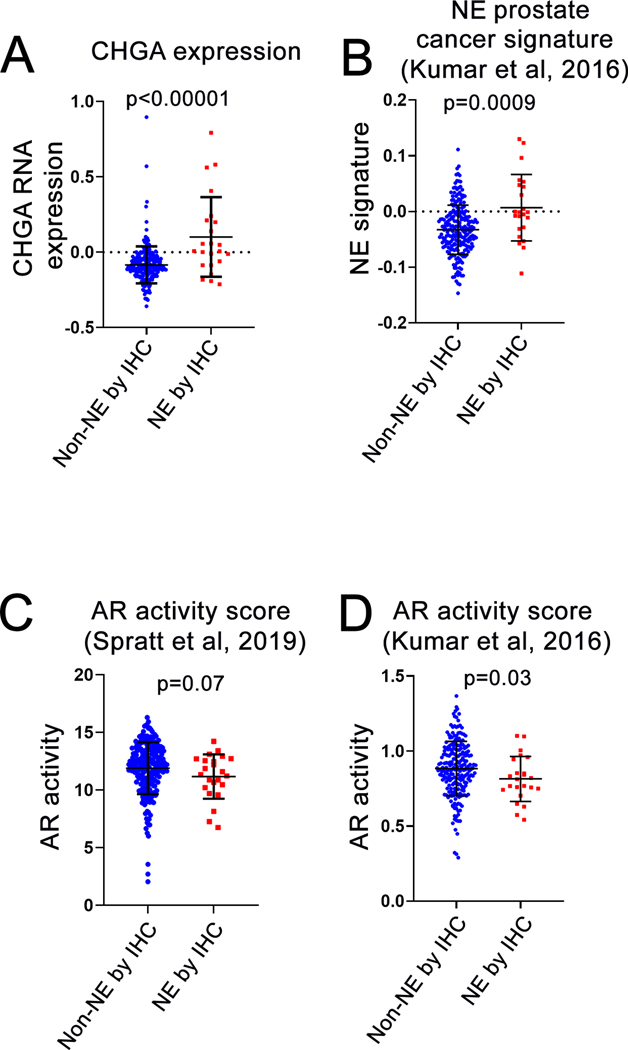
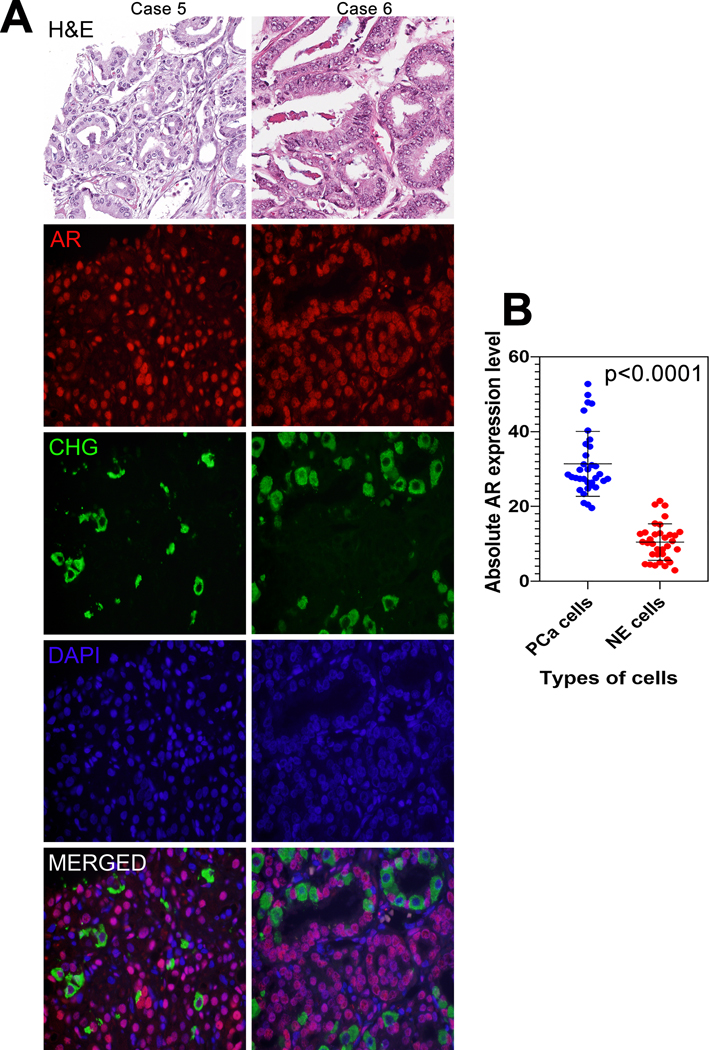
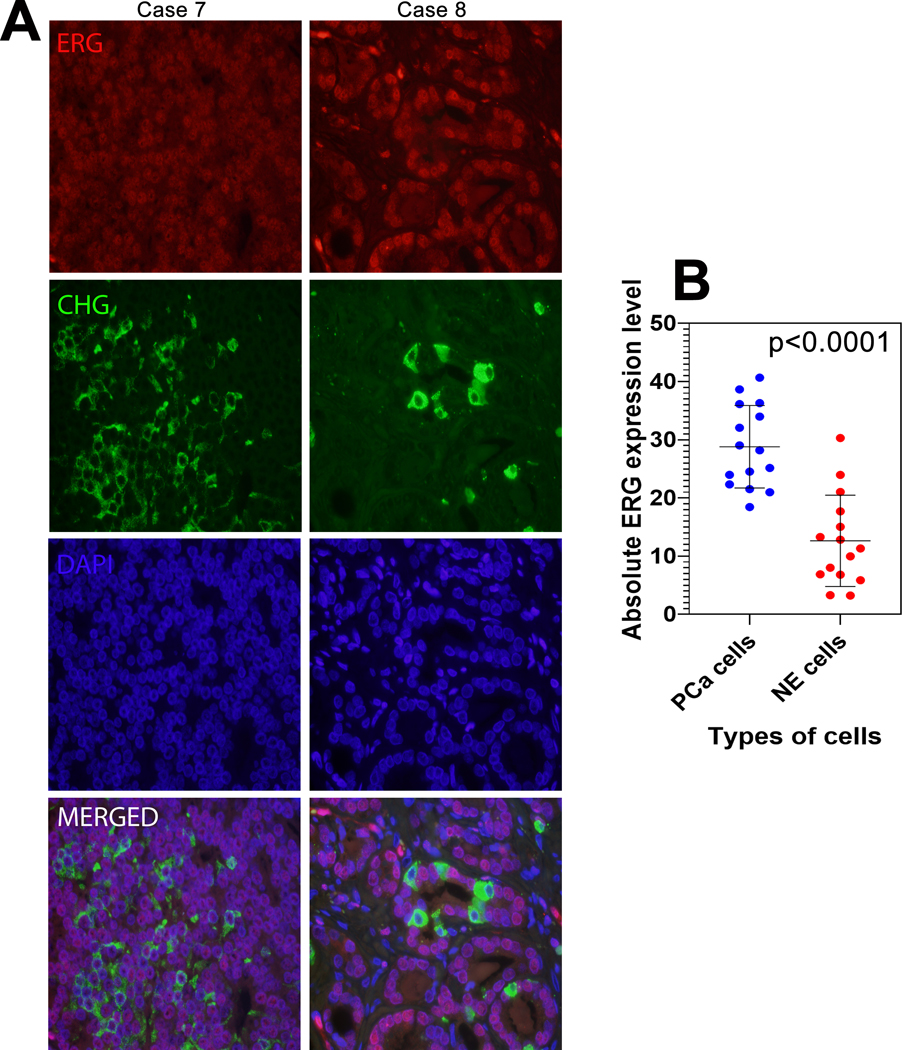
Benign NE cells expressed significantly lower quantified AR levels compared with paired benign luminal cells (P < .001). Similarly, paneth-like NE carcinoma cells or carcinoma cells expressing chromogranin A expressed significantly lower quantified AR levels than paired non-NE carcinoma cells (P < .001). Quantified ERG protein expression, was also lower in chromogranin A-labeled adenocarcinoma cells compared with unlabeled cells (P < .001) and tumors with NE differentiation showed lower gene expression scores for AR activity compared with those without. Despite evidence of lower AR signaling, adenocarcinomas with NE differentiation did not differ by prevalence of TP53 missense mutations, or PTEN or RB1 loss, compared with those without NE differentiation. Finally, NE differentiation was not associated with time to metastasis in intermediate- and high-risk patients (P = .6 on multivariate analysis), nor with progression-free survival in patients with CRPC treated with abiraterone or enzalutamide (P = .9).
NE differentiation in usual-type primary prostate adenocarcinoma is a molecularly and clinically distinct form of lineage plasticity from that occurring in small cell NE carcinoma.
前列腺小细胞神经内分泌(NE)癌经典地失去雄激素受体(AR)表达,可能存在 RB1、TP53 和 PTEN 肿瘤抑制基因的丢失,并且与预后不良相关。然而,通常型腺癌也可能包含神经内分泌分化区域,在这种情况下,分子特征和生物学意义不太确定。
我们使用三个独立的研究集检查了具有≥5%神经内分泌分化的原发性前列腺腺癌的分子表型和肿瘤学结果(在组织微阵列上的任何给定肿瘤点上,≥5%的嗜铬粒蛋白 A 阳性神经内分泌细胞):一组具有 Paneth 细胞样神经内分泌分化的肿瘤(n=26)、一组中间和高危患者的回顾性病例队列,这些患者的不良结局丰富(n=267)和一组来自接受阿比特龙或恩扎鲁胺治疗的最终去势抵抗转移性前列腺癌(CRPC)男性的原发性肿瘤的回顾性系列(n=55)。
良性 NE 细胞表达的定量 AR 水平明显低于配对的良性 luminal 细胞(P<0.001)。同样,Paneth 样神经内分泌癌细胞或表达嗜铬粒蛋白 A 的癌细胞表达的定量 AR 水平明显低于配对的非神经内分泌癌细胞(P<0.001)。与未标记的细胞相比,在嗜铬粒蛋白 A 标记的腺癌细胞中,定量 ERG 蛋白表达也较低(P<0.001),并且具有神经内分泌分化的肿瘤的 AR 活性基因表达评分低于没有神经内分泌分化的肿瘤。尽管 AR 信号转导较低,但与没有神经内分泌分化的肿瘤相比,具有神经内分泌分化的腺癌在 TP53 错义突变的流行率或 PTEN 或 RB1 缺失方面没有差异。最后,在中间和高危患者中,神经内分泌分化与转移时间无关(多变量分析 P=0.6),在接受阿比特龙或恩扎鲁胺治疗的 CRPC 患者中,与无进展生存期也无关(P=0.9)。
在通常型原发性前列腺腺癌中,神经内分泌分化是与小细胞 NE 癌中发生的谱系可塑性在分子和临床上不同的形式。