Department of Psychiatry, Corporal Michael J. Crescenz VA Medical Center and the Perelman School of Medicine at the University of Pennsylvania, 3900 Woodland Avenue, Philadelphia, PA, 19104, USA.
Analysis Group, 111 Huntington Ave, Boston, MA, 02199, USA.
BMC Psychiatry. 2020 Jul 11;20(1):365. doi: 10.1186/s12888-020-02748-0.
The relative benefits and risks of long-term maintenance treatment with antipsychotics have not been well studied in patients with bipolar disorder and major depressive disorder. For example, while antipsychotic dose reduction has been recommended in the management of serious side effects associated with antipsychotics, there is limited evidence on the impact of lowering doses on the course of underlying mood disorders.
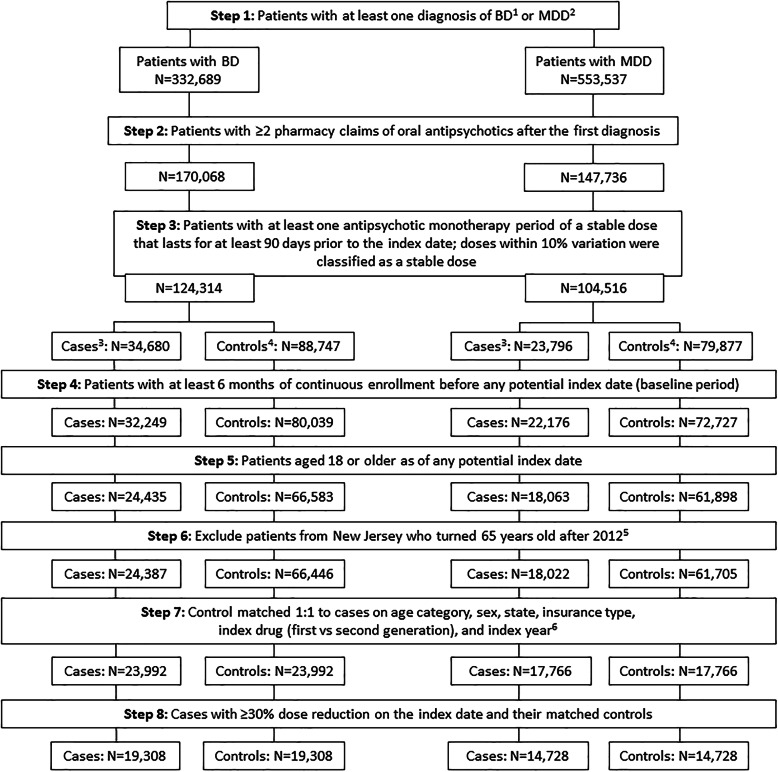
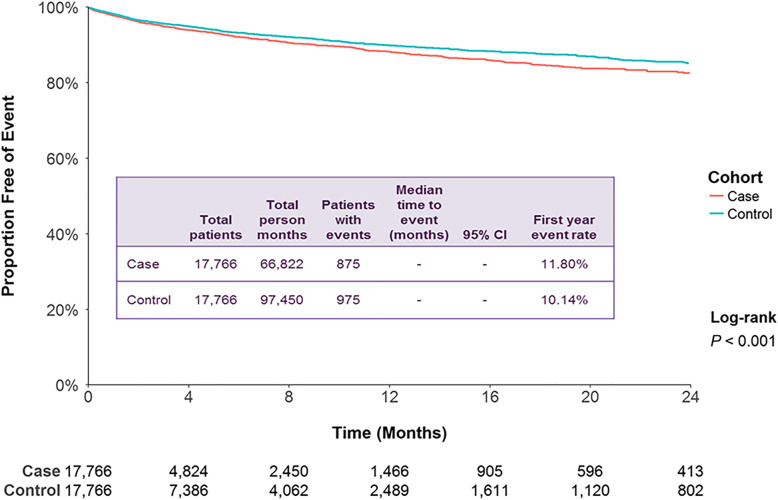
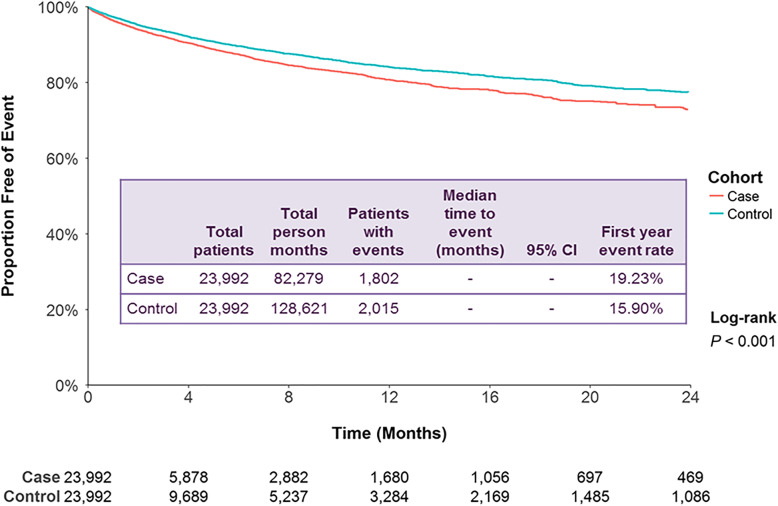
This retrospective cohort study analyzed the impact of antipsychotic dose reduction in patients with bipolar disorder or major depressive disorder. Medical claims from six US states over a 6-year period were analyzed for patients with ≥10% or ≥ 30% reductions in antipsychotic dose (cases) and compared using survival analyses with matched controls receiving a stable dosage. Outcomes included hospitalizations for disease-specific mood disorders, other psychiatric disorders and all-cause emergency room visits, and claims for tardive dyskinesia.
A total of 23,992 patients with bipolar disorder and 17,766 with major depressive disorder had a ≥ 10% dose reduction, while 19,308 and 14,728, respectively, had a ≥ 30% dose reduction. In multivariate analyses, cases with a ≥ 10% dose reduction had a significantly increased risk of disease-specific admission (bipolar disorder: hazard ratio [95% confidence interval], 1.22 [1.15-1.31]; major depressive disorder: 1.22 [1.11-1.34]), other psychiatric admission (bipolar disorder: 1.19 [1.13-1.24]; major depressive disorder: 1.17 [1.11-1.23]), all-cause admission (bipolar disorder: 1.17 [1.12-1.23]; major depressive disorder: 1.11 [1.05-1.16]), and all-cause emergency room visits (bipolar disorder: 1.09 [1.05-1.13]; major depressive disorder: 1.07 [1.02-1.11]) (all P < 0.01). Similar results were observed following an ≥30% dose reduction. Dose reduction was not associated with decreased claims for tardive dyskinesia.
Patients with mood disorders who had antipsychotic dose reductions showed small but statistically significant increases in all-cause and mental health-related hospitalizations, which may lead to increased healthcare costs. These results highlight the need for additional long-term studies of the necessity and safety of maintenance antipsychotic treatment in mood disorders.
在双相情感障碍和重性抑郁障碍患者中,长期维持抗精神病药物治疗的相对益处和风险尚未得到充分研究。例如,虽然已经建议减少抗精神病药物剂量以管理与抗精神病药物相关的严重副作用,但关于降低剂量对潜在心境障碍病程的影响的证据有限。
本回顾性队列研究分析了双相情感障碍或重性抑郁障碍患者减少抗精神病药物剂量的影响。对 6 个美国州在 6 年期间的医疗索赔数据进行了分析,以确定抗精神病药物剂量减少≥10%或≥30%的患者(病例),并使用生存分析与接受稳定剂量的匹配对照进行比较。结局包括心境障碍、其他精神障碍和全因急诊就诊的特定疾病住院治疗,以及迟发性运动障碍的索赔。
共有 23992 例双相情感障碍患者和 17766 例重性抑郁障碍患者的抗精神病药物剂量减少≥10%,而分别有 19308 例和 14728 例患者的抗精神病药物剂量减少≥30%。多变量分析显示,抗精神病药物剂量减少≥10%的病例发生特定疾病入院的风险显著增加(双相情感障碍:风险比[95%置信区间],1.22[1.15-1.31];重性抑郁障碍:1.22[1.11-1.34]),其他精神科入院(双相情感障碍:1.19[1.13-1.24];重性抑郁障碍:1.17[1.11-1.23]),全因入院(双相情感障碍:1.17[1.12-1.23];重性抑郁障碍:1.11[1.05-1.16]),以及全因急诊就诊(双相情感障碍:1.09[1.05-1.13];重性抑郁障碍:1.07[1.02-1.11])(均 P<0.01)。观察到剂量减少≥30%后也有类似的结果。抗精神病药物剂量减少与迟发性运动障碍索赔的减少无关。
抗精神病药物剂量减少的心境障碍患者全因和精神健康相关住院治疗的增加虽小但具有统计学意义,这可能导致医疗保健成本增加。这些结果强调了需要进一步开展长期研究,以确定心境障碍维持抗精神病药物治疗的必要性和安全性。