Soter Center for Women's Cardiovascular Research, Leon H. Charney Division of Cardiology, Department of Medicine, New York University School of Medicine, New York, New York.
Department of Medicine, New York University School of Medicine, New York, New York.
JACC Cardiovasc Imaging. 2020 Sep;13(9):1906-1913. doi: 10.1016/j.jcmg.2020.02.037. Epub 2020 Jul 9.
The aim of this study was to determine the prevalence of myocarditis among patients presenting with myocardial infarction with nonobstructive coronary arteries (MINOCA) in relation to the angiographic severity of nonobstructive coronary artery disease (CAD).
MINOCA represents about 6% of all cases of acute myocardial infarction. Myocarditis is a diagnosis that may be identified by cardiac magnetic resonance (CMR) imaging in patients with a provisional diagnosis of MINOCA.
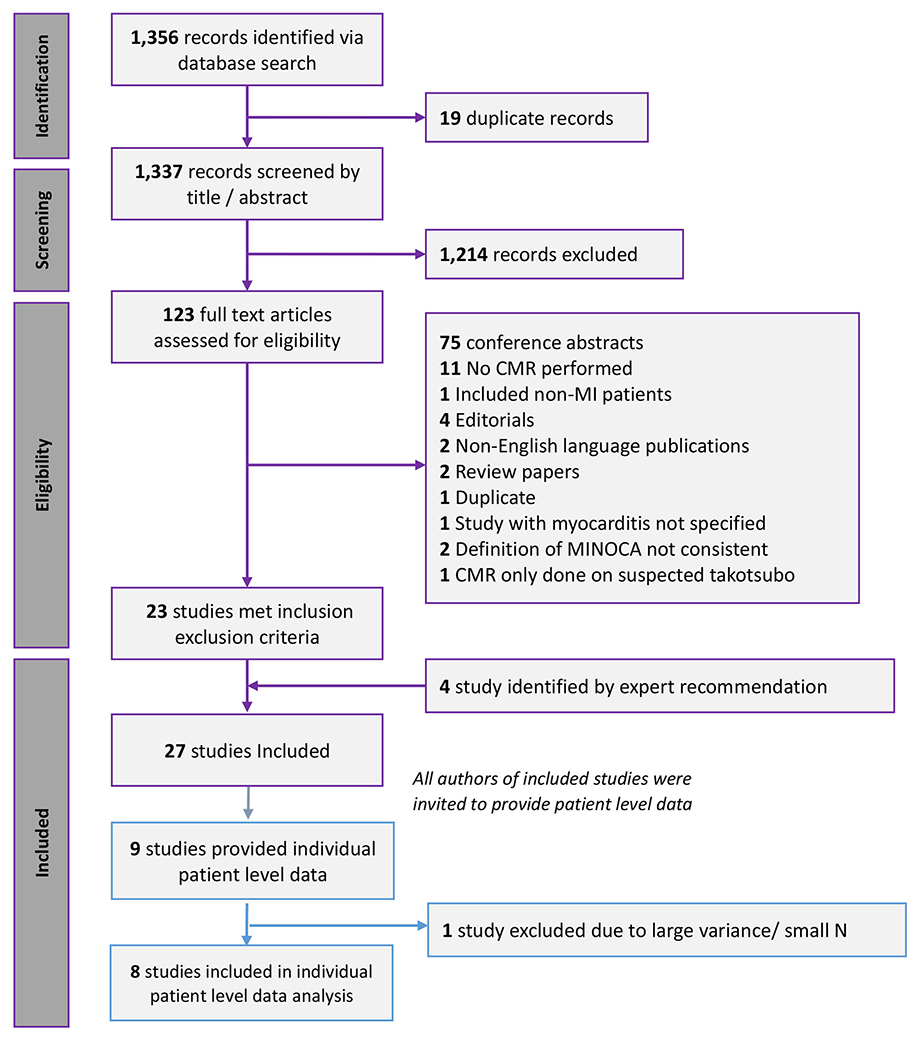
A systematic review was performed to identify studies reporting the results of CMR findings in MINOCA patients with nonobstructive CAD or normal coronary arteries. Study-level and individual patient data meta-analyses were performed using fixed- and random-effects methods.
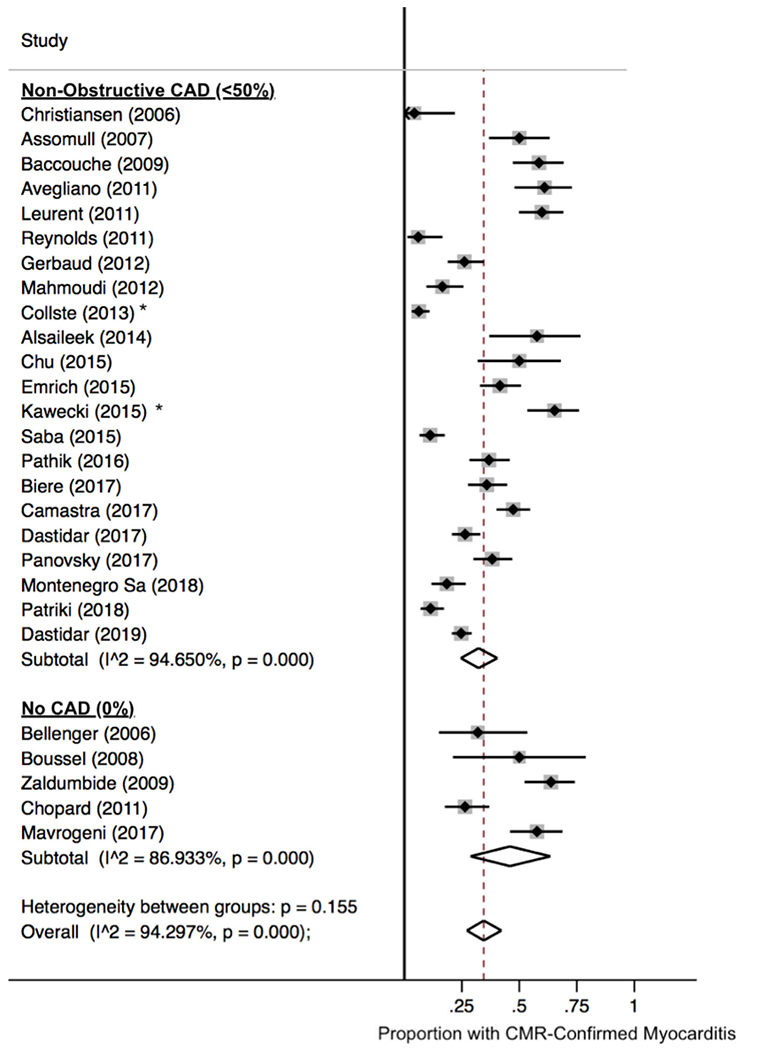
Twenty-seven papers were included, with 2,921 patients with MINOCA; CMR findings were reported in 2,866 (98.1%). Myocarditis prevalence was 34.5% (95% confidence interval [CI]: 27.2% to 42.2%) overall and was numerically higher in studies that defined MINOCA as myocardial infarction with angiographically normal coronary arteries compared with a definition that permitted nonobstructive CAD (45.9% vs. 32.3%; p = 0.16). In a meta-analysis of individual patient data from 9 of the 27 studies, the pooled prevalence of CMR-confirmed myocarditis was greater in patients with angiographically normal coronary arteries than in those with nonobstructive CAD (51% [95% CI: 47% to 56%] vs. 23% [95% CI: 18% to 27%]; p < 0.001). Men and younger patients with MINOCA were more likely to have myocarditis. Angiographically normal coronary arteries were associated with increased odds of myocarditis after adjustment for age and sex (adjusted odds ratio: 2.30; 95% CI: 1.12 to 4.71; p = 0.023).
Patients with a provisional diagnosis of MINOCA are more likely to have CMR findings consistent with myocarditis if they have angiographically normal coronary arteries.
本研究旨在确定非阻塞性冠状动脉疾病(CAD)患者中,以非阻塞性冠状动脉狭窄严重程度为参照,出现心肌梗死且无阻塞性冠状动脉的患者(MINOCA)中心肌炎的发生率。
MINOCA 约占所有急性心肌梗死病例的 6%。对于疑似 MINOCA 的患者,心脏磁共振(CMR)成像有助于明确心肌炎的诊断。
我们进行了系统综述,以确定报告非阻塞性 CAD 或正常冠状动脉的 MINOCA 患者 CMR 结果的研究。使用固定效应和随机效应方法进行研究水平和个体患者数据的荟萃分析。
共纳入 27 篇文献,纳入 2921 例 MINOCA 患者;其中 2866 例(98.1%)报告了 CMR 结果。总体上,心肌炎的发生率为 34.5%(95%置信区间:27.2%至 42.2%),根据心肌梗死伴血管造影正常冠状动脉的定义,MINOCA 患者的发生率高于允许非阻塞性 CAD 的定义(45.9%比 32.3%;p=0.16)。在 27 项研究中的 9 项的个体患者数据的荟萃分析中,与非阻塞性 CAD 相比,血管造影正常冠状动脉的患者 CMR 确诊心肌炎的发生率更高(51%[95%置信区间:47%至 56%]比 23%[95%置信区间:18%至 27%];p<0.001)。MINOCA 患者中,男性和年轻患者更有可能发生心肌炎。在调整年龄和性别后,血管造影正常的冠状动脉与心肌炎的发生几率增加相关(调整后的优势比:2.30;95%置信区间:1.12 至 4.71;p=0.023)。
对于疑似 MINOCA 的患者,如果其存在血管造影正常的冠状动脉,则更有可能通过 CMR 检查发现符合心肌炎的结果。