Hsia Brian C, Greige Nicolas, Quiroz Jose A, Khokhar Ahmed S, Daily Johanna, Di Biase Luigi, Ferrick Kevin J, Fisher John D, Krumerman Andrew
Division of Cardiology, Department of Medicine, Albert Einstein College of Medicine & Montefiore Medical Center, 111 East 210th Street, Room N2, Bronx, NY, 10467, USA.
Harold and Muriel Block Institute for Clinical and Translational Research, Albert Einstein College of Medicine & Montefiore Medical Center, Bronx, NY, USA.
J Interv Card Electrophysiol. 2020 Nov;59(2):337-345. doi: 10.1007/s10840-020-00822-x. Epub 2020 Jul 11.
Hydroxychloroquine, chloroquine, and azithromycin have been used for treatment of COVID-19, but may cause QT prolongation. Minority populations are disproportionately impacted by COVID-19. This study evaluates the risk of QT prolongation and subsequent outcomes after administration of these medications in largely underrepresented minority COVID-19 patients.
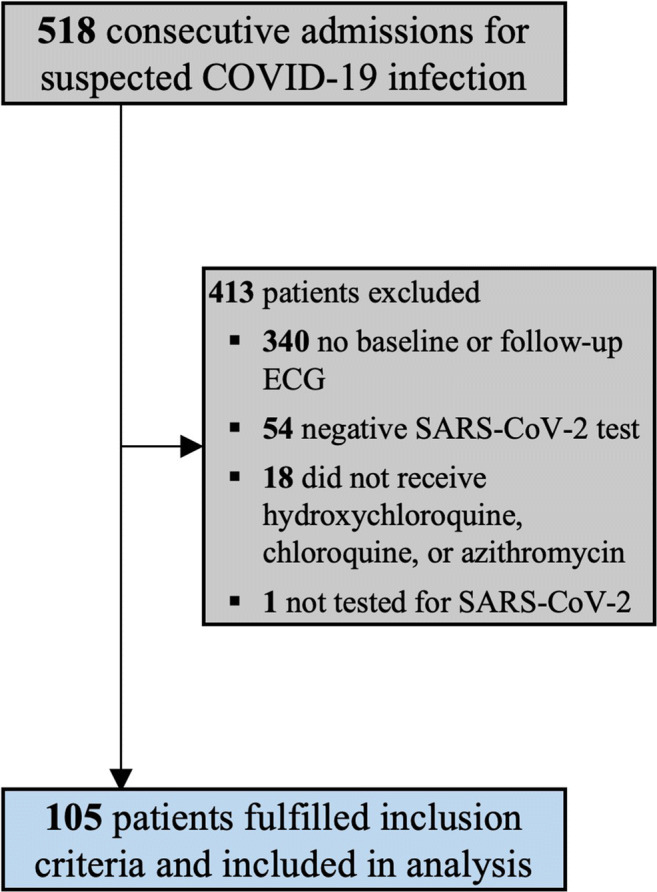
We conducted an observational study on hospitalized COVID-19 patients in the Montefiore Health System (Bronx, NY). We examined electrocardiograms (ECG) pre/post-medication initiation to evaluate QTc, HR, QRS duration, and presence of other arrhythmias.
One hundred five patients (mean age 67 years; 44.8% F) were analyzed. The median time from the first dose of any treatment to post-medication ECG was 2 days (IQR: 1-3). QTc in men increased from baseline (440 vs 455 ms, p < 0.001), as well as in women (438 vs 463 ms, p < 0.001). The proportion of patients with QT prolongation increased significantly (14.3% vs 34.3%, p < 0.001) even when adjusted for electrolyte abnormalities. The number of patients whose QTc > 500 ms was significantly increased after treatment (16.2% vs. 4.8%, p < 0.01). Patients with either QTc > 500 ms or an increase of 60 ms had a higher frequency of death (47.6% vs. 22.6%, p = 0.02) with an odds ratio of 3.1 (95% CI: 1.1-8.7). Adjusting for race/ethnicity yielded no significant associations.
Hydroxychloroquine, chloroquine, and/or azithromycin were associated with QTc prolongation but did not result in fatal arrhythmias. Our findings suggest that any harm is unlikely to outweigh potential benefits of treatment. Careful risk-benefit analyses for individual patients should guide the use of these medications. Randomized control trials are necessary to evaluate their efficacies.
羟氯喹、氯喹和阿奇霉素已被用于治疗2019冠状病毒病(COVID-19),但可能导致QT间期延长。少数族裔受COVID-19的影响尤为严重。本研究评估了在代表性严重不足的少数族裔COVID-19患者中使用这些药物后QT间期延长的风险及后续结果。
我们对蒙特菲奥里医疗系统(纽约州布朗克斯)的住院COVID-19患者进行了一项观察性研究。我们检查了用药前/用药后的心电图(ECG),以评估QTc、心率、QRS波时限以及是否存在其他心律失常。
共分析了105例患者(平均年龄67岁;44.8%为女性)。从首次服用任何治疗药物到用药后心电图检查的中位时间为2天(四分位间距:1 - 3天)。男性的QTc较基线水平升高(440 vs 455毫秒,p < 0.001),女性也是如此(438 vs 463毫秒,p < 0.001)。即使校正了电解质异常,QT间期延长的患者比例仍显著增加(14.3% vs 34.3%,p < 0.001)。治疗后QTc > 500毫秒的患者数量显著增加(16.2% vs 4.8%,p < 0.01)。QTc > 500毫秒或增加60毫秒的患者死亡频率更高(47.6% vs 22.6%,p = 0.02),优势比为3.1(95%置信区间:1.1 - 8.7)。校正种族/族裔因素后未发现显著关联。
羟氯喹、氯喹和/或阿奇霉素与QTc延长有关,但未导致致命性心律失常。我们的研究结果表明,任何危害都不太可能超过治疗的潜在益处。对个体患者进行仔细的风险效益分析应指导这些药物的使用。有必要进行随机对照试验来评估它们的疗效。