Kakked Gaurav, Salameh Habeeb, Cheesman Antonio R, Kumta Nikhil A, Nagula Satish, DiMaio Christopher J
Department of Medicine, Mount Sinai St. Luke's/West Hospitals, New York, USA.
Dr. Henry D. Janowitz Division of Gastroenterology, Mount Sinai Hospital, Icahn School of Medicine at Mount Sinai, New York, USA.
Endosc Ultrasound. 2020 Sep-Oct;9(5):298-307. doi: 10.4103/eus.eus_10_20.
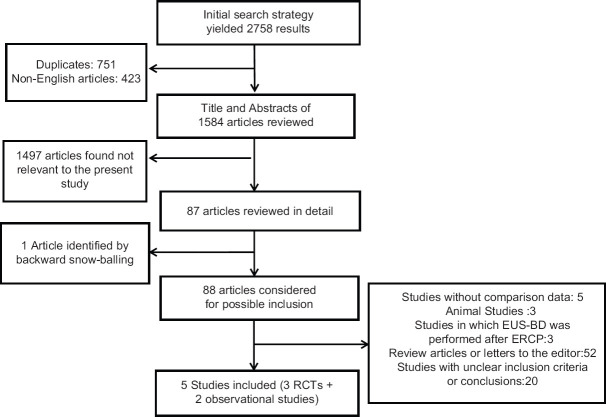
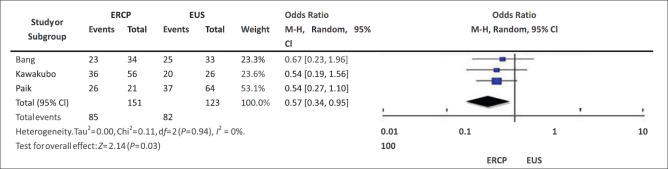
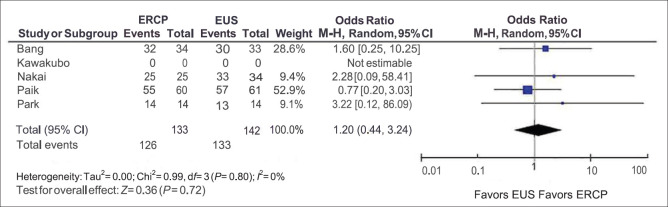
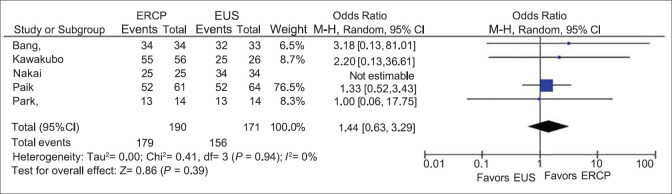
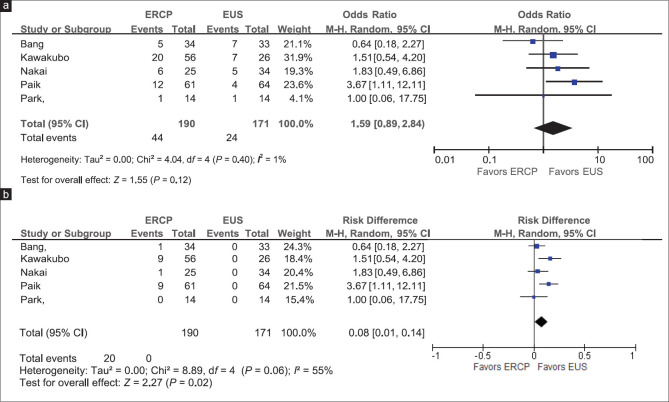
EUS-guided biliary drainage (EUS-BD) has been used as a salvage modality for relief of malignant biliary obstruction (MBO) after a failed ERCP. Multiple recent randomized controlled trials (RCTs) and observational studies have been published to assess the suitability of EUS-BD as a first-line modality for achieving palliative BD. We aimed to perform a systematic review and meta-analysis comparing primary EUS-BD versus ERCP for MBO. We searched PubMed, Medline, and Embase up to January 1, 2019, to identify RCTs and observational studies evaluating the efficacy and safety of primary EUS-BD (without a prior attempted ERCP) versus ERCP. Quality of RCTs and observational studies was assessed using Jadad and Newcastle-Ottawa scores, respectively. The outcomes of interest were technical success, clinical success, odds of requiring a repeat intervention, and procedure-related adverse events. Odds ratios (ORs) and standard mean difference were calculated for categorical and continuous variables, respectively. Meta-analysis was performed using the random effects model in RevMan 5.3 (the Cochrane Collaboration, the Nordic Cochrane Centre, Copenhagen, Denmark). Five studies (three RCTs and two observational studies) with 361 patients were included. Both procedures achieved comparable technical success (OR: 1.20 [0.44-3.24], I = 0%) and clinical success (OR: 1.44, confidence interval [CI]: 0.63-3.29, I = 0%). The overall adverse outcomes (OR: 1.59 [0.89-2.84]) did not differ between the two groups. In the ERCP group, 9.5% of patients developed procedure-related pancreatitis versus zero in the EUS group (risk difference = 0.08%, P = 0.02). There was no statistically significant difference in nonpancreatitis-related adverse events. The odds of requiring reintervention for BD (1.68 [0.76-3.73], I = 42%) did not differ significantly. The ERCP group had significantly higher odds of requiring reintervention due to tumor overgrowth (5.35 [1.64-17.50], I = 0%). EUS-BD has comparable technical and clinical success to ERCP and can potentially be used as a first-line palliative modality for MBO where expertise is available. ERCP-related pancreatitis which can cause significant morbidity can be completely avoided with EUS.
内镜超声引导下胆道引流术(EUS-BD)已被用作在ERCP失败后缓解恶性胆道梗阻(MBO)的挽救性治疗手段。最近发表了多项随机对照试验(RCT)和观察性研究,以评估EUS-BD作为实现姑息性胆道引流一线治疗手段的适用性。我们旨在进行一项系统评价和荟萃分析,比较原发性EUS-BD与ERCP治疗MBO的效果。我们检索了截至2019年1月1日的PubMed、Medline和Embase,以确定评估原发性EUS-BD(未事先尝试ERCP)与ERCP疗效和安全性的RCT和观察性研究。分别使用Jadad评分和纽卡斯尔-渥太华评分评估RCT和观察性研究的质量。感兴趣的结局包括技术成功率、临床成功率、需要重复干预的几率以及与手术相关的不良事件。分别计算分类变量和连续变量的比值比(OR)和标准平均差。使用RevMan 5.3(Cochrane协作网北欧Cochrane中心,丹麦哥本哈根)中的随机效应模型进行荟萃分析。纳入了五项研究(三项RCT和两项观察性研究),共361例患者。两种手术在技术成功率(OR:1.20[0.44-3.24],I²=0%)和临床成功率(OR:1.44,置信区间[CI]:0.63-3.29,I²=0%)方面相当。两组的总体不良结局(OR:1.59[0.89-2.84])没有差异。在ERCP组中,9.5%的患者发生了与手术相关的胰腺炎,而EUS组为零(风险差异=0.08%,P=0.02)。在与胰腺炎无关的不良事件方面没有统计学显著差异。因胆道引流需要再次干预的几率(1.68[0.76-3.73],I²=42%)没有显著差异。ERCP组因肿瘤过度生长需要再次干预的几率显著更高(5.35[1.64-17.50],I²=0%)。EUS-BD在技术和临床成功率方面与ERCP相当,在有专业技术的情况下,有可能作为MBO的一线姑息性治疗手段。EUS可以完全避免ERCP相关的胰腺炎,而这种胰腺炎可导致严重的发病情况。