Anyanwu Philip Emeka, Pouwels Koen, Walker Anne, Moore Michael, Majeed Azeem, Hayhoe Benedict W J, Tonkin-Crine Sarah, Borek Aleksandra, Hopkins Susan, Mcleod Monsey, Costelloe Céire
Department of Primary Care and Public Health, Imperial College London, London, UK
Nuffield Department of Population Health, Health Economics Research Centre, University of Oxford, Oxford, UK.
BJGP Open. 2020 Aug 25;4(3). doi: 10.3399/bjgpopen20X101052. Print 2020 Aug.
In 2017, approximately 73% of antibiotics in England were prescribed from primary care practices. It has been estimated that 9%-23% of antibiotic prescriptions between 2013 and 2015 were inappropriate. Reducing antibiotic prescribing in primary care was included as one of the national priorities in a financial incentive scheme in 2015-2016.
To investigate whether the effects of the Quality Premium (QP), which provided performance-related financial incentives to clinical commissioning groups (CCGs), could be explained by practice characteristics that contribute to variations in antibiotic prescribing.
DESIGN & SETTING: Longitudinal monthly prescribing data were analysed for 6251 primary care practices in England from April 2014 to March 2016.
Linear generalised estimating equations models were fitted, examining the effect of the 2015-2016 QP on the number of antibiotic items per specific therapeutic group age-sex related prescribing unit (STAR-PU) prescribed, adjusting for seasonality and months since implementation. Consistency of effects after further adjustment for variations in practice characteristics were also examined, including practice workforce, comorbidities prevalence, prescribing rates of non-antibiotic drugs, and deprivation.
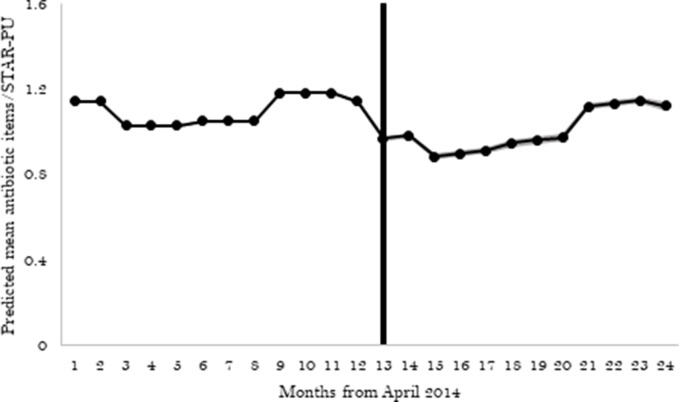
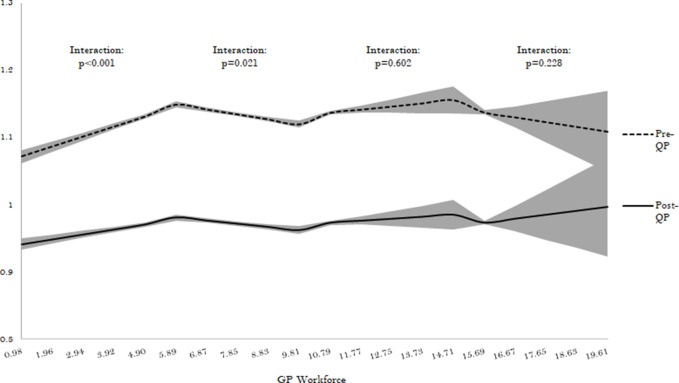
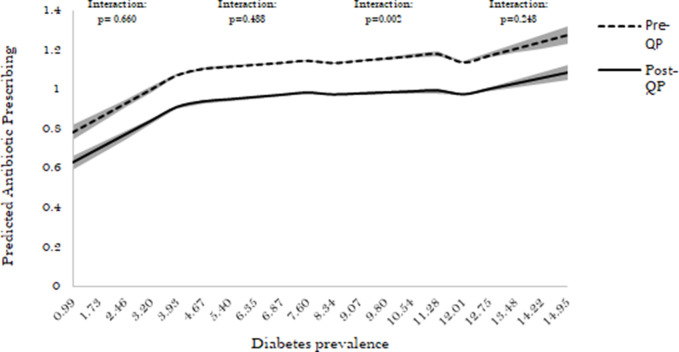
Antibiotics prescribed in primary care practices in England reduced by -0.172 items per STAR-PU (95% confidence interval [CI] = -0.180 to -0.171) after 2015-2016 QP implementation, with slight increases in the months following April 2015 (+0.014 items per STAR-PU; 95% CI = +0.013 to +0.014). Adjusting the model for practice characteristics, the immediate and month-on-month effects following implementation remained consistent, with slight attenuation in immediate reduction from -0.172 to -0.166 items per STAR-PU. In subgroup analysis, the QP effect was significantly greater among the top 20% prescribing practices (interaction <0.001). Practices with low workforce and those with higher diabetes prevalence had greater reductions in prescribing following 2015-2016 QP compared with other practices (interaction <0.001).
In high-prescribing practices, those with low workforce and high diabetes prevalence had more reduction following the QP compared with other practices, highlighting the need for targeted support of these practices and appropriate resourcing of primary care.
2017年,英格兰约73%的抗生素是由基层医疗诊所开出的。据估计,2013年至2015年间,9%-23%的抗生素处方是不恰当的。在2015 - 2016年的一项财政激励计划中,减少基层医疗中的抗生素处方被列为国家优先事项之一。
调查为临床委托小组(CCG)提供与绩效相关财政激励的质量奖励(QP)的效果,是否可以由导致抗生素处方差异的诊所特征来解释。
分析了2014年4月至2016年3月期间英格兰6251家基层医疗诊所的纵向月度处方数据。
拟合线性广义估计方程模型,研究2015 - 2016年QP对每个特定治疗组年龄 - 性别相关处方单位(STAR - PU)开出的抗生素项目数量的影响,并对季节性和实施后的月份进行调整。还检查了在进一步调整诊所特征差异(包括诊所工作人员、合并症患病率、非抗生素药物处方率和贫困程度)后的效果一致性。
2015 - 2016年QP实施后,英格兰基层医疗诊所开出的抗生素数量减少了 - 0.172项/STAR - PU(95%置信区间[CI] = - 0.180至 - 0.171),在2015年4月后的几个月略有增加(+0.014项/STAR - PU;95% CI = +0.013至 +0.014)。对诊所特征调整模型后,实施后的即时和逐月效果保持一致,即时减少量略有减弱,从 - 0.172项/STAR - PU降至 - 0.166项/STAR - PU。在亚组分析中,在处方量最高的20%的诊所中,QP效果显著更大(交互作用<0.001)。与其他诊所相比,工作人员较少且糖尿病患病率较高的诊所在2015 - 2016年QP实施后处方量减少更多(交互作用<0.001)。
在高处方量诊所中,与其他诊所相比,工作人员少且糖尿病患病率高的诊所在QP实施后减少量更多,这突出表明需要对这些诊所提供有针对性的支持,并为基层医疗提供适当的资源。