Zhang Jian-Wei, Cai Yue, Xie Xiao-Yu, Hu Hua-Bin, Ling Jia-Yu, Wu Ze-Hua, Lan Ping, Wu Xiao-Jian, Huang Mei-Jin, Wang Hui, Kang Liang, Zhou Zhi-Yang, Wang Jian-Ping, Deng Yan-Hong
Department of Medical Oncology, The Sixth Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, P. R. China.
Guangdong Provincial Key Laboratory of Colorectal and Pelvic Floor Diseases, Guangzhou, Guangdong, P. R. China.
Gastroenterol Rep (Oxf). 2020 Feb 8;8(3):234-241. doi: 10.1093/gastro/goz073. eCollection 2020 Jun.
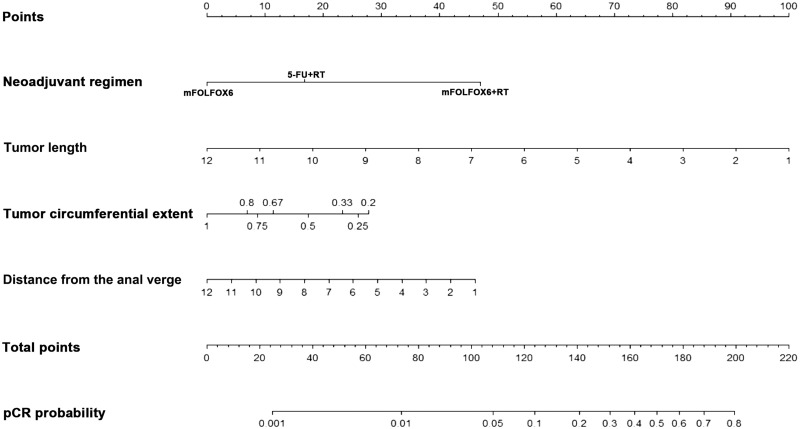
Preoperative fluoropyrimidine with radiotherapy was regarded as the standard of care for locally advanced rectal cancer (LARC). The model for predicting pCR in LARC patients was based on standard treatment only. This study aimed to establish a nomogram with pretherapeutic parameters and different neoadjuvant regimens for predicting pathologic complete response (pCR) and tumor downstaging or good response (ypT0-2N0M0) after receiving neoadjuvant treatment in patients with LARC based on a randomized clinical trial.
Between January 2011 and February 2015, 309 patients with rectal cancer were enrolled from a prospective randomized study (NCT01211210). All pretreatment clinical parameters were collected to build a nomogram for predicting pCR and tumor downstaging. The model was subjected to bootstrap internal validation. The predictive performance of the model was assessed with concordance index (C-index) and calibration plots.
Of the 309 patients, 53 (17.2%) achieved pCR and 132 (42.7%) patients were classified as tumor downstaging with ypT0-2N0M0. Based on the logistic-regression analysis and clinical consideration, tumor length ( = 0.005), tumor circumferential extent ( = 0.036), distance from the anal verge ( = 0.019), and neoadjuvant treatment regimen ( < 0.001) showed independent association with pCR following neoadjuvant treatment. The tumor length ( = 0.015), tumor circumferential extent ( = 0.001), distance from the anal verge ( = 0.032), clinical T category ( = 0.012), and neoadjuvant treatment regimen ( = 0.001) were significantly associated with good tumor downstaging (ypT0-2N0M0). Nomograms were developed to predict the probability of pCR and tumor downstaging with a C-index of 0.802 (95% confidential interval [CI], 0.736-0.867) and 0.730 (95% CI, 0.672-0.784). Internal validation revealed good performance of the calibration plots.
The nomogram provided individual prediction responses to different preoperative treatment for patients with rectal cancer. This model might help physicians in selecting an optimized treatment, but warrants further external validation.
术前氟尿嘧啶联合放疗曾被视为局部晚期直肠癌(LARC)的标准治疗方案。预测LARC患者病理完全缓解(pCR)的模型仅基于标准治疗。本研究旨在基于一项随机临床试验,建立一个包含治疗前参数和不同新辅助治疗方案的列线图,用于预测LARC患者接受新辅助治疗后的病理完全缓解(pCR)以及肿瘤降期或良好反应(ypT0 - 2N0M0)。
2011年1月至2015年2月期间,从一项前瞻性随机研究(NCT01211210)中纳入309例直肠癌患者。收集所有治疗前临床参数以构建预测pCR和肿瘤降期的列线图。该模型进行了自助法内部验证。通过一致性指数(C指数)和校准图评估模型的预测性能。
309例患者中,53例(17.2%)达到pCR,132例(42.7%)患者被分类为ypT0 - 2N0M0的肿瘤降期。基于逻辑回归分析和临床考虑,肿瘤长度(P = 0.005)、肿瘤周径范围(P = 0.036)、距肛缘距离(P = 0.019)和新辅助治疗方案(P < 0.001)显示与新辅助治疗后的pCR独立相关。肿瘤长度(P = 0.015)、肿瘤周径范围(P = 0.001)、距肛缘距离(P = 0.032)、临床T分期(P = 0.012)和新辅助治疗方案(P = 0.001)与良好的肿瘤降期(ypT0 - 2N0M0)显著相关。建立了列线图以预测pCR和肿瘤降期的概率,C指数分别为0.802(95%置信区间[CI],0.736 - 0.867)和0.730(95%CI,0.672 - 0.784)。内部验证显示校准图性能良好。
列线图为直肠癌患者不同术前治疗提供了个体预测反应。该模型可能有助于医生选择优化治疗方案,但需要进一步的外部验证。