Kleindienst Andrea, Georgiev Simeon, Schlaffer Sven Martin, Buchfelder Michael
Department of Neurosurgery, Friedrich-Alexander-University Nürnberg-Erlangen, Erlangen, Germany.
J Endocr Soc. 2020 Jun 9;4(7):bvaa068. doi: 10.1210/jendso/bvaa068. eCollection 2020 Jul 1.
The relevance of hyponatremia has been acknowledged by guidelines from the United States (2013) and Europe (2014). However, treatment recommendations differ due to limited evidence.
In hyponatremia following pituitary surgery-caused by the syndrome of inappropriate antidiuretic hormone (SIADH) secretion-we compared fluid restriction with the pharmacological increase of water excretion by blocking the vasopressin 2 receptors with tolvaptan at a low and a moderate dose.
Prospective observational study.
Neurosurgical Department of a University hospital with more than 200 surgical pituitary procedures per year.
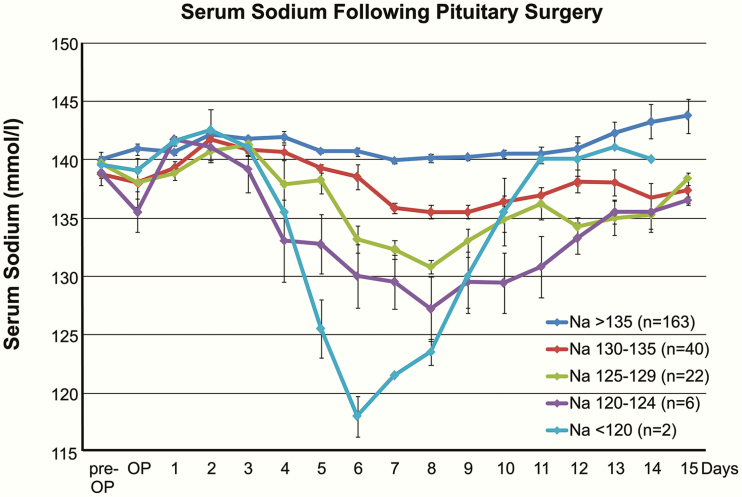
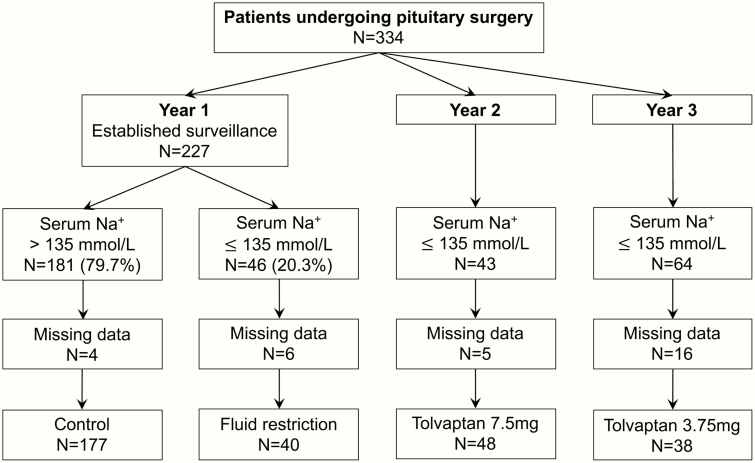
Patients undergoing pituitary surgery and developing serum sodium below 136 mmol/L. The diagnosis of SIADH was established by euvolemia (daily measurement of body weight and fluid balance), inappropriately concentrated urine (specific gravity), and exclusion of adrenocorticotropic and thyroid-stimulating hormone deficiency.
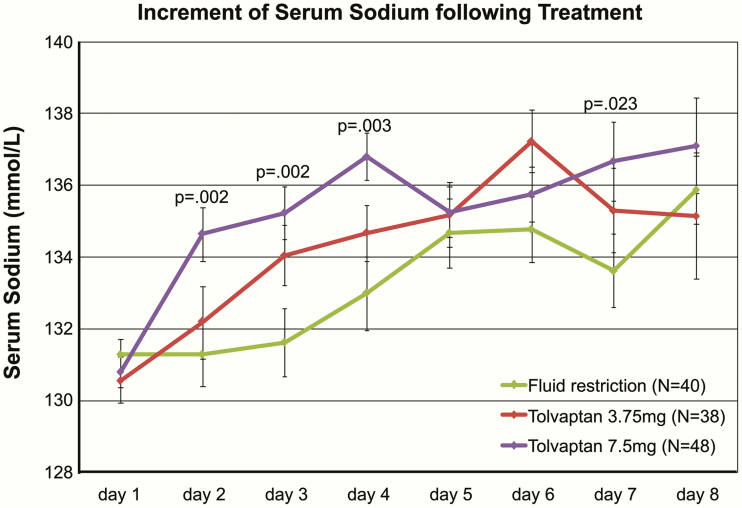
Patients were treated with fluid restriction (n = 40) or tolvaptan at 3.75 (n = 38) or 7.5 mg (n = 48).
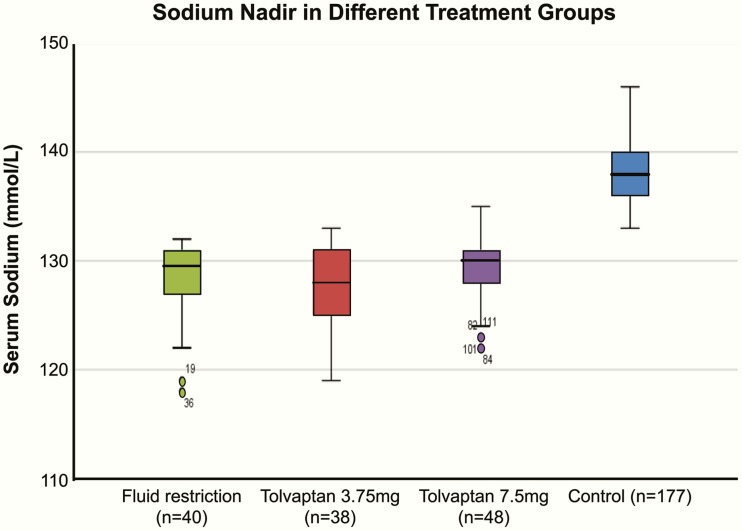
Treatment efficacy was assessed by the duration of hyponatremia, sodium nadir, and length of hospitalization. Safety was established by a sodium increment below 10 mmol/L per day and exclusion of side effects.
Treatment with 7.5 mg of tolvaptan resulted in a significant attenuation of hyponatremia and in a significant overcorrection of serum sodium in 30% of patients. The duration of hospitalization did not differ between treatment groups.
Tolvaptan at a moderate dose is more effective than fluid restriction in the treatment of SIADH. Overcorrection of serum sodium may be a side effect of tolvaptan even at low doses.
美国(2013年)和欧洲(2014年)的指南已认可低钠血症的相关性。然而,由于证据有限,治疗建议存在差异。
在垂体手术后因抗利尿激素分泌不当综合征(SIADH)导致的低钠血症中,我们比较了液体限制与使用低剂量和中等剂量托伐普坦阻断血管加压素2受体以增加水排泄的药物治疗效果。
前瞻性观察研究。
一家每年进行200多例垂体手术的大学医院神经外科。
接受垂体手术且血清钠低于136 mmol/L的患者。通过血容量正常(每日测量体重和液体平衡)、尿液过度浓缩(比重)以及排除促肾上腺皮质激素和促甲状腺激素缺乏来确诊SIADH。
患者接受液体限制治疗(n = 40)或服用3.75 mg(n = 38)或7.5 mg(n = 48)的托伐普坦。
通过低钠血症持续时间、最低血钠值和住院时间评估治疗效果。通过每日血钠升高低于10 mmol/L以及排除副作用来确定安全性。
服用7.5 mg托伐普坦治疗导致低钠血症显著减轻,30%的患者血清钠出现显著纠正过度。各治疗组之间住院时间无差异。
中等剂量的托伐普坦在治疗SIADH方面比液体限制更有效。即使是低剂量的托伐普坦,血清钠纠正过度也可能是其副作用。