Department of Respiratory Oncology, Guangxi Medical University Affiliated Tumor Hospital, Nanning City, Guangxi Zhuang Autonomous Region, China.
Department of No.5 Chemotherapy, Guangxi Medical University Affiliated Tumor Hospital, Nanning City, Guangxi Zhuang Autonomous Region, China.
Cancer Med. 2020 Sep;9(17):6268-6280. doi: 10.1002/cam4.3244. Epub 2020 Jul 21.
To investigate the relation between AAPR and OS in patients with advanced non-small cell lung cancer (NSCLC).
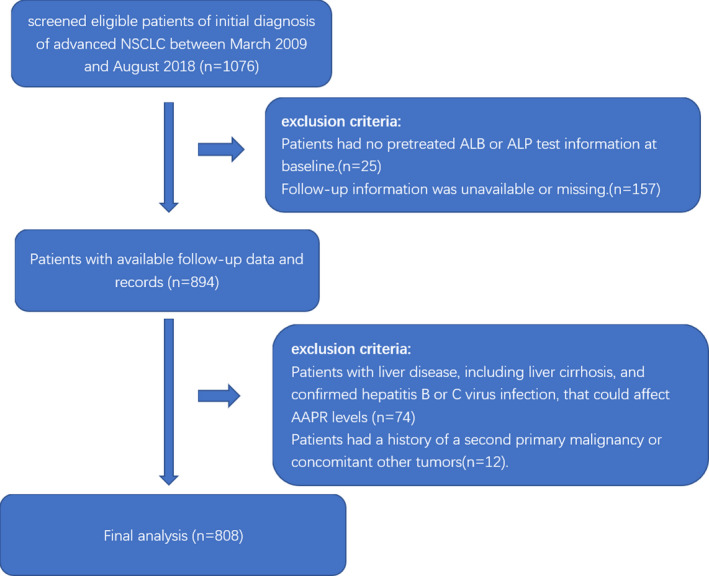
A retrospective cohort study was conducted with 808 patients with advanced NSCLC who were treated in Guangxi Medical University Affiliated Tumor Hospital in China from 5 March 2009 to 31 August 2018. The target-independent and dependent variables were AAPR measured in patients before anticancer treatment and overall survival (OS), respectively. Covariates involved in this study included age, gender, ECOG status, smoking history, clinical stages, pathological type, driver mutation (EGFR or ALK), metastasis or not (bone, lung, liver, brain, malignant plural effusion, and other organs), number of organ metastasis(≤3, >3), first-line regiment and number of treatment lines (≤3, >3).
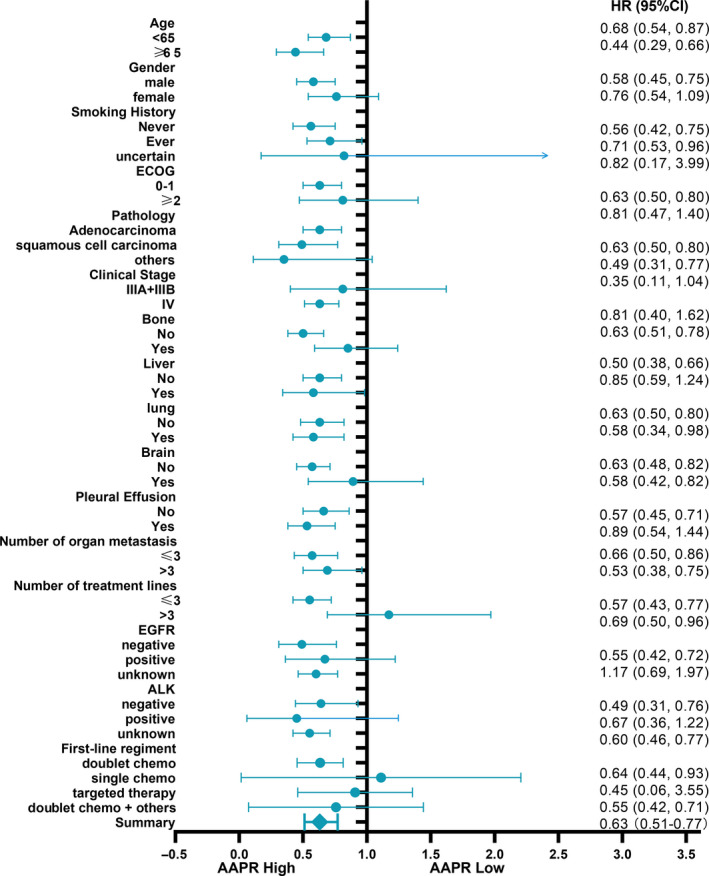
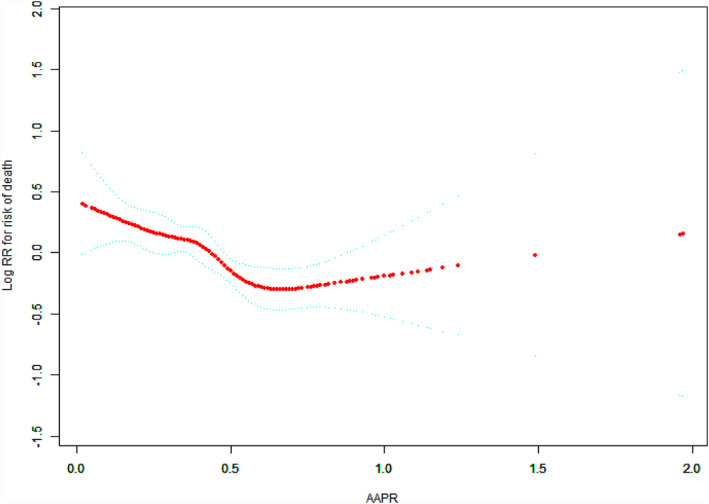
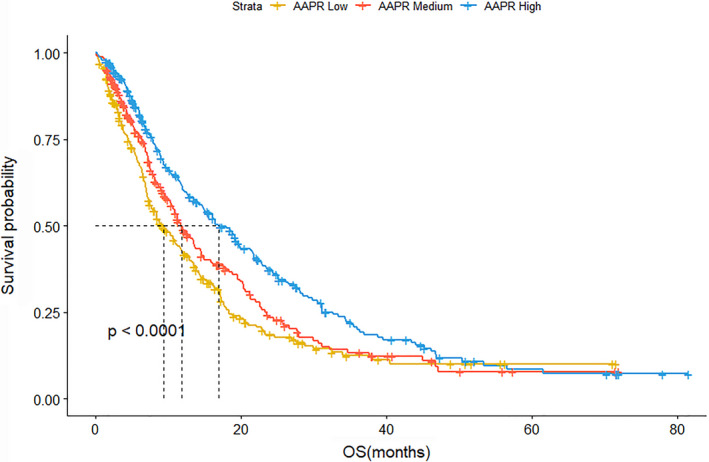
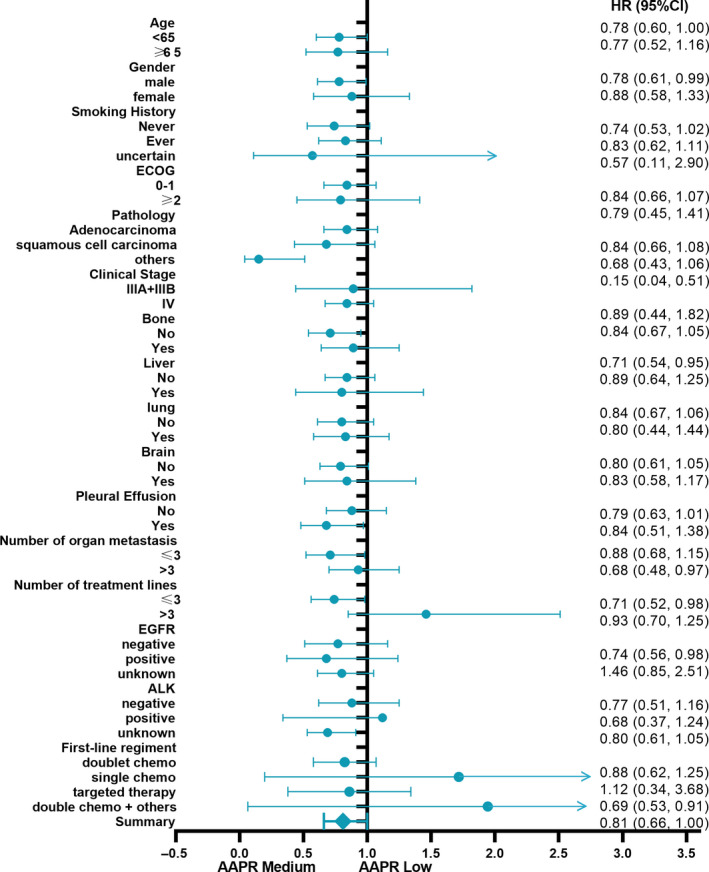
The mean age of the selected patients was 58.3 ± 10.9 years and 68.6% were male. We divided patients according to their AAPR into low (AAPR < 0.34, n = 266), medium (AAPR = 0.34-0.47, n = 259), and high (AAPR > 0.47, n = 283) tertile groups. Medium and high AAPR were associated with a decreased risk of death after fully adjusted Cox proportional hazard model(s) with hazards ratio (HR) 0.77 (95%CI = 0.58-1.03) and HR 0.59 (95%CI = 0.45-0.78), respectively (P for trend <.05). The median OS of low, medium, and high AAPR was 9.3, 11.8, and 16.9 months, respectively (P value <.0001). No optimal cutoff value of AAPR for prognosing OS was identified by smooth curve fitting. The HR and the 95% confidence intervals of the left and right sides of the inflection point 0.6 as cutoff value were 0.28 (95%CI = 0.14-0.57) and 0.77 (95%CI = 0.34-1.73), respectively (P value = .127). By subgroup analysis, similar results were consistently observed across nearly all the subgroups.
Our study implied that pretreatment AAPR can be used as an independent prognostic factor in patients with advanced NSCLC. This ratio should be applied for risk stratification and clinical decision-making in those patients.
研究晚期非小细胞肺癌(NSCLC)患者中 AAPR 与 OS 的关系。
采用回顾性队列研究,纳入 2009 年 3 月 5 日至 2018 年 8 月 31 日在广西医科大学附属肿瘤医院接受治疗的 808 例晚期 NSCLC 患者。无目标依赖和依赖变量分别为患者接受抗癌治疗前的 AAPR 和总生存(OS)。本研究的协变量包括年龄、性别、ECOG 状态、吸烟史、临床分期、病理类型、驱动突变(EGFR 或 ALK)、转移或不转移(骨、肺、肝、脑、恶性胸腔积液和其他器官)、转移器官数量(≤3、>3)、一线方案和治疗线数(≤3、>3)。
入选患者的平均年龄为 58.3±10.9 岁,68.6%为男性。我们根据 AAPR 将患者分为低(AAPR<0.34,n=266)、中(AAPR=0.34-0.47,n=259)和高(AAPR>0.47,n=283)三分位组。在经过完全调整的 Cox 比例风险模型后,中、高 AAPR 与死亡风险降低相关,风险比(HR)分别为 0.77(95%CI=0.58-1.03)和 0.59(95%CI=0.45-0.78)(P 趋势<0.05)。低、中、高 AAPR 的中位 OS 分别为 9.3、11.8 和 16.9 个月(P 值<0.0001)。通过平滑曲线拟合,未确定 AAPR 预测 OS 的最佳截断值。拐点 0.6 左侧和右侧的 HR 及其 95%置信区间分别为 0.28(95%CI=0.14-0.57)和 0.77(95%CI=0.34-1.73)(P 值=0.127)。通过亚组分析,几乎所有亚组均观察到相似的结果。
本研究表明,治疗前 AAPR 可作为晚期 NSCLC 患者的独立预后因素。该比值可用于这些患者的风险分层和临床决策。