Zhao Zhi-Ming, Jiang Nan, Gao Yuan-Xing, Yin Zhu-Zeng, Zhao Guo-Dong, Tan Xiang-Long, Xu Yong, Liu Rong
Second Department of Hepatopancreatobiliary Surgery, The First Medical Center of Chinese PLA General Hospital, Beijing 100853, China.
World J Gastrointest Oncol. 2020 Jun 15;12(6):642-650. doi: 10.4251/wjgo.v12.i6.642.
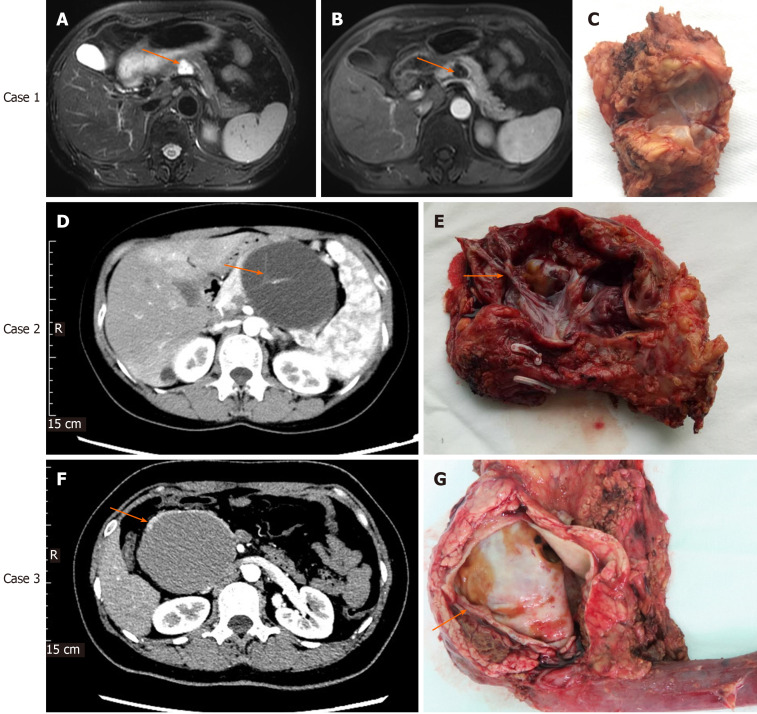
Mucinous cystic neoplasm (MCN) of the pancreas is characterized by mucin-producing columnar epithelium and dense ovarian-type stroma and at risk for malignant transformation. Early diagnosis and treatment of MCN are particularly important.
To investigate the clinical characteristics of and management strategies for pancreatic mucinous cystadenoma (MCA) and mucinous cystadenocarcinoma (MCC).
The clinical and pathological data of 82 patients with pancreatic MCA and MCC who underwent surgical resection at our department between April 2015 and March 2019 were retrospectively analyzed.
Of the 82 patients included in this study, 70 had MCA and 12 had MCC. Tumor size of MCC was larger than that of MCA ( = 0.049). Age and serum levels of tumor markers carcinoembryonic antigen (CEA), carbohydrate antigen (CA) 19-9, and CA12-5 were significantly higher in MCC than in MCA patients ( = 0.005, 0.026, and 0.037, respectively). MCA tumor size was positively correlated with serum CA19-9 levels ( = 0.389, = 0.001). Compared with MCC, MCA had a higher minimally invasive surgery rate ( = 0.014). In the MCA group, the rate of major complications was 5.7% and that of clinically relevant pancreatic fistula was 8.6%; the corresponding rates in the MCC group were 16.7% and 16.7%, respectively.
Tumor size, age, and serum CEA, CA19-9, and CA12-5 levels may contribute to management of patients with MCN. Surgical resection is the primary treatment modality for MCC and MCA.
胰腺黏液性囊性肿瘤(MCN)以产生黏液的柱状上皮和致密的卵巢型间质为特征,有恶变风险。MCN的早期诊断和治疗尤为重要。
探讨胰腺黏液性囊腺瘤(MCA)和黏液性囊腺癌(MCC)的临床特征及治疗策略。
回顾性分析2015年4月至2019年3月在我科接受手术切除的82例胰腺MCA和MCC患者的临床和病理资料。
本研究纳入的82例患者中,70例为MCA,12例为MCC。MCC的肿瘤大小大于MCA(P = 0.049)。MCC患者的年龄以及肿瘤标志物癌胚抗原(CEA)、糖类抗原(CA)19-9和CA12-5的血清水平显著高于MCA患者(分别为P = 0.005、0.026和0.037)。MCA肿瘤大小与血清CA19-9水平呈正相关(r = 0.389,P = 0.001)。与MCC相比,MCA的微创手术率更高(P = 0.014)。在MCA组中,主要并发症发生率为5.7%,临床相关胰瘘发生率为8.6%;MCC组相应发生率分别为16.7%和16.7%。
肿瘤大小、年龄以及血清CEA、CA19-9和CA12-5水平可能有助于MCN患者的管理。手术切除是MCC和MCA的主要治疗方式。