Department of Molecular Genetics and Microbiology, Duke University School of Medicine, Durham, NC, 27705, USA.
Neurovascular Surgery Program, Department of Neurosurgery, University of Chicago Medicine and Biological Sciences, Chicago, IL, 60637, USA.
Angiogenesis. 2020 Nov;23(4):651-666. doi: 10.1007/s10456-020-09736-8. Epub 2020 Jul 24.
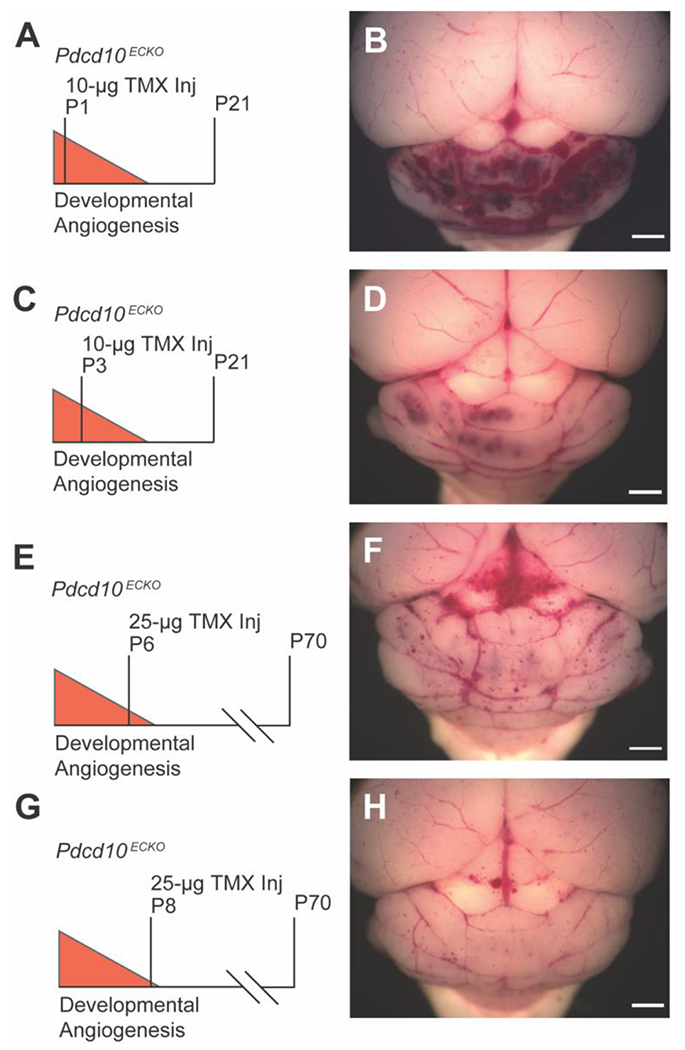
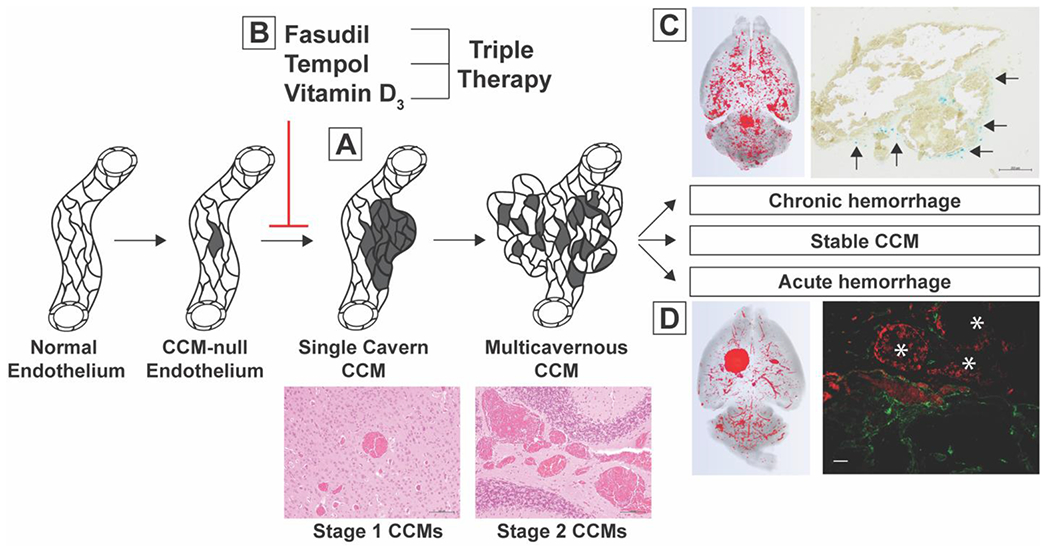
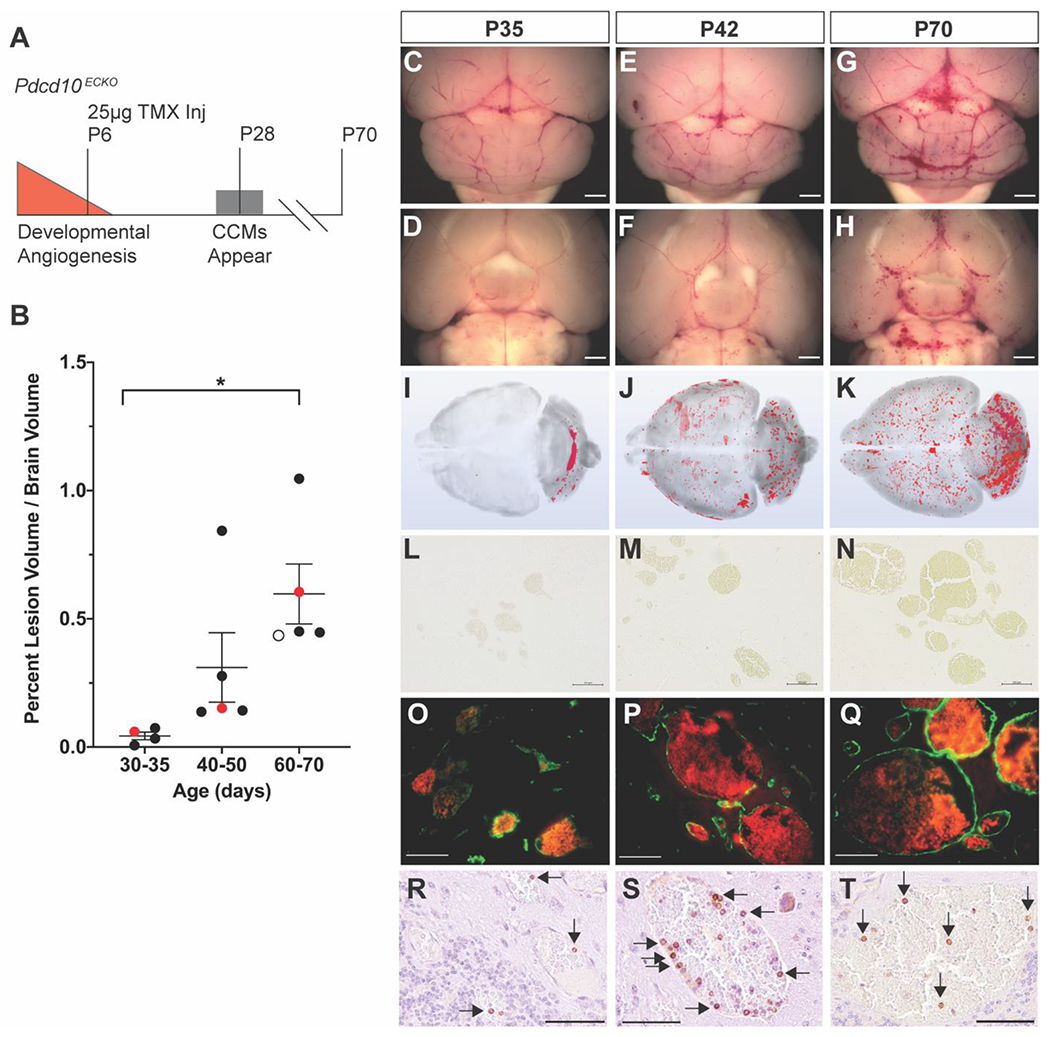
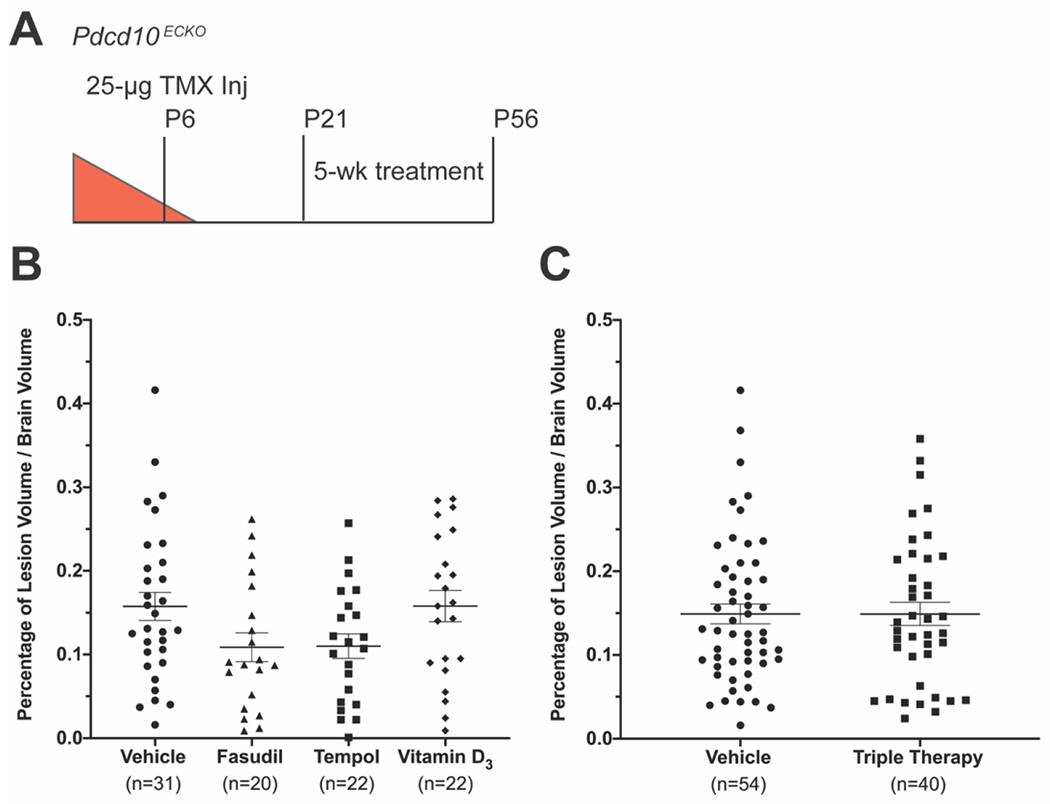
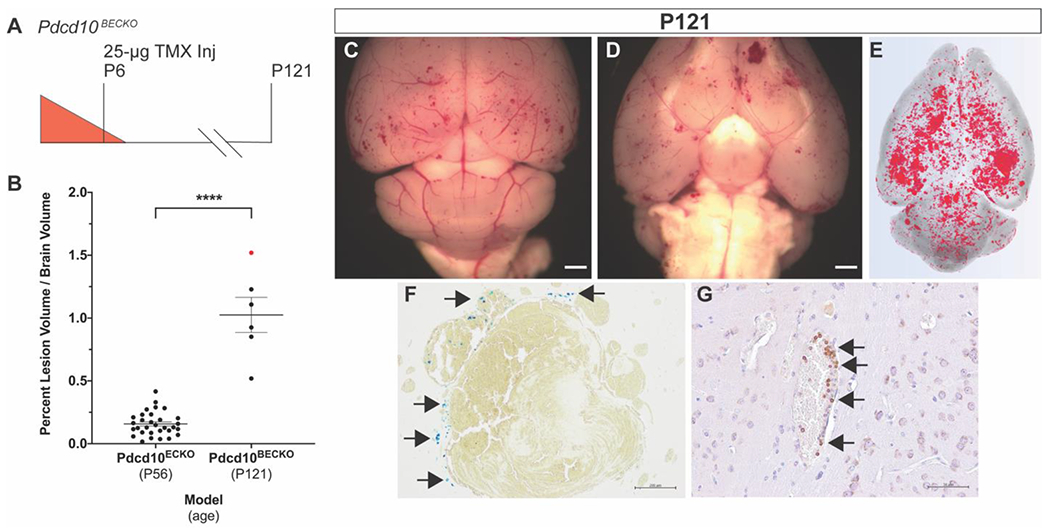
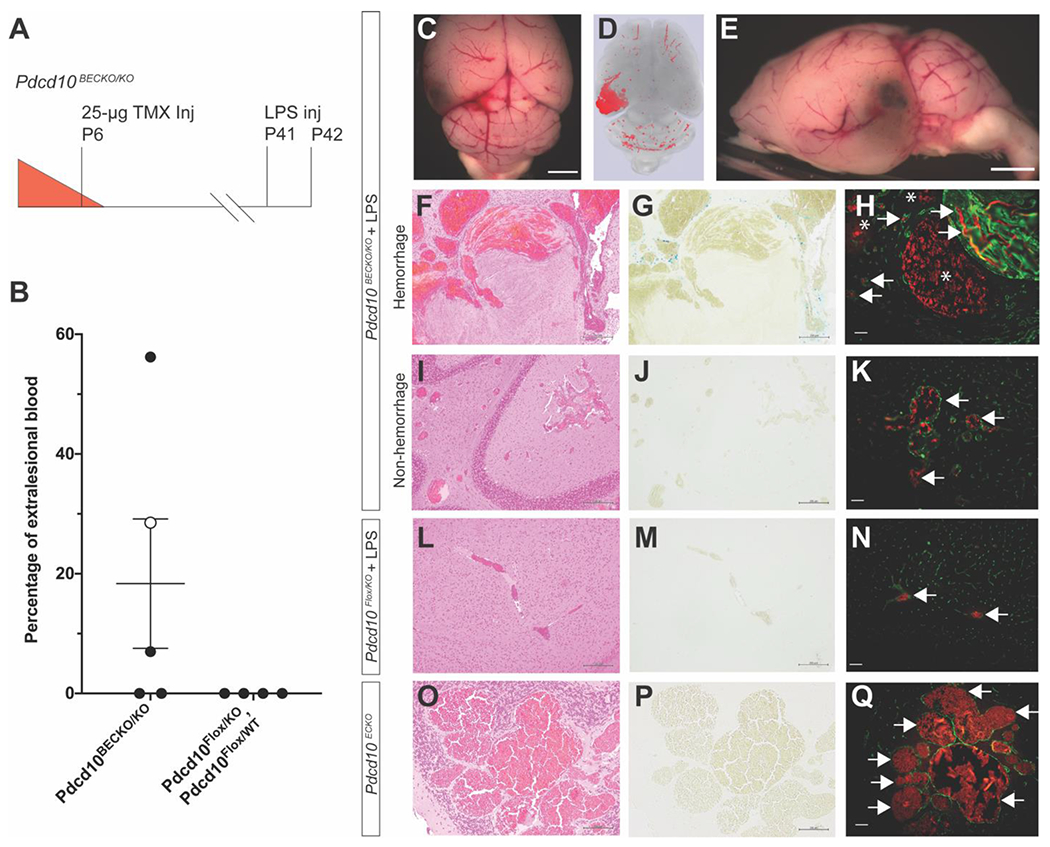
Cerebral cavernous malformations (CCMs) are ectatic capillary-venous malformations that develop in approximately 0.5% of the population. Patients with CCMs may develop headaches, focal neurologic deficits, seizures, and hemorrhages. While symptomatic CCMs, depending upon the anatomic location, can be surgically removed, there is currently no pharmaceutical therapy to treat CCMs. Several mouse models have been developed to better understand CCM pathogenesis and test therapeutics. The most common mouse models induce a large CCM burden that is anatomically restricted to the cerebellum and contributes to lethality in the early days of life. These inducible models thus have a relatively short period for drug administration. We developed an inducible CCM3 mouse model that develops CCMs after weaning and provides a longer period for potential therapeutic intervention. Using this new model, three recently proposed CCM therapies, fasudil, tempol, vitamin D, and a combination of the three drugs, failed to substantially reduce CCM formation when treatment was administered for 5 weeks, from postnatal day 21 (P21) to P56. We next restricted Ccm3 deletion to the brain vasculature and provided greater time (121 days) for CCMs to develop chronic hemorrhage, recapitulating the human lesions. We also developed the first model of acute CCM hemorrhage by injecting mice harboring CCMs with lipopolysaccharide. These efficient models will enable future drug studies to more precisely target clinically relevant features of CCM disease: CCM formation, chronic hemorrhage, and acute hemorrhage.
脑内海绵状血管畸形(CCMs)是一种扩张的毛细血管-静脉畸形,约占人口的 0.5%。CCMs 患者可能会出现头痛、局灶性神经功能缺损、癫痫发作和出血。虽然有症状的 CCMs 根据解剖位置可以通过手术切除,但目前尚无药物治疗方法。已经开发了几种小鼠模型来更好地了解 CCM 发病机制并测试治疗方法。最常见的小鼠模型诱导大量 CCM 负担,解剖上局限于小脑,并导致生命早期的致死性。因此,这些诱导型模型用于药物给药的时间相对较短。我们开发了一种诱导型 CCM3 小鼠模型,该模型在断奶后会发展出 CCMs,并为潜在的治疗干预提供了更长的时间。使用这种新模型,三种最近提出的 CCM 治疗方法(法舒地尔、替米沙坦、维生素 D 以及三种药物的联合应用)在从出生后第 21 天(P21)至 P56 的 5 周治疗期间未能显著减少 CCM 的形成。接下来,我们将 Ccm3 缺失限制在脑血管中,并提供更长的时间(121 天)让 CCMs 发展慢性出血,重现人类病变。我们还通过向携带 CCM 的小鼠注射脂多糖来开发急性 CCM 出血的首个模型。这些高效模型将使未来的药物研究能够更精确地针对 CCM 疾病的临床相关特征:CCM 的形成、慢性出血和急性出血。