Centre de Référence des Maladies Trophoblastiques, Lyon, France.
Université de Lyon, Université Claude Bernard Lyon 1, Faculté de Médecine Lyon-Sud, CICLY, Lyon, France.
J Clin Oncol. 2020 Sep 20;38(27):3129-3137. doi: 10.1200/JCO.20.00803. Epub 2020 Jul 27.
Women with gestational trophoblastic tumors (GTT) resistant to single-agent chemotherapy receive alternative chemotherapy regimens, which, although effective, cause considerable toxicity. All GTT subtypes express programmed death-ligand 1 (PD-L1), and natural killer (NK) cells are involved in trophoblast immunosurveillance. Avelumab (anti-PD-L1) induces NK cell-mediated cytotoxicity. The TROPHIMMUN trial assessed avelumab in women with chemotherapy-resistant GTT.
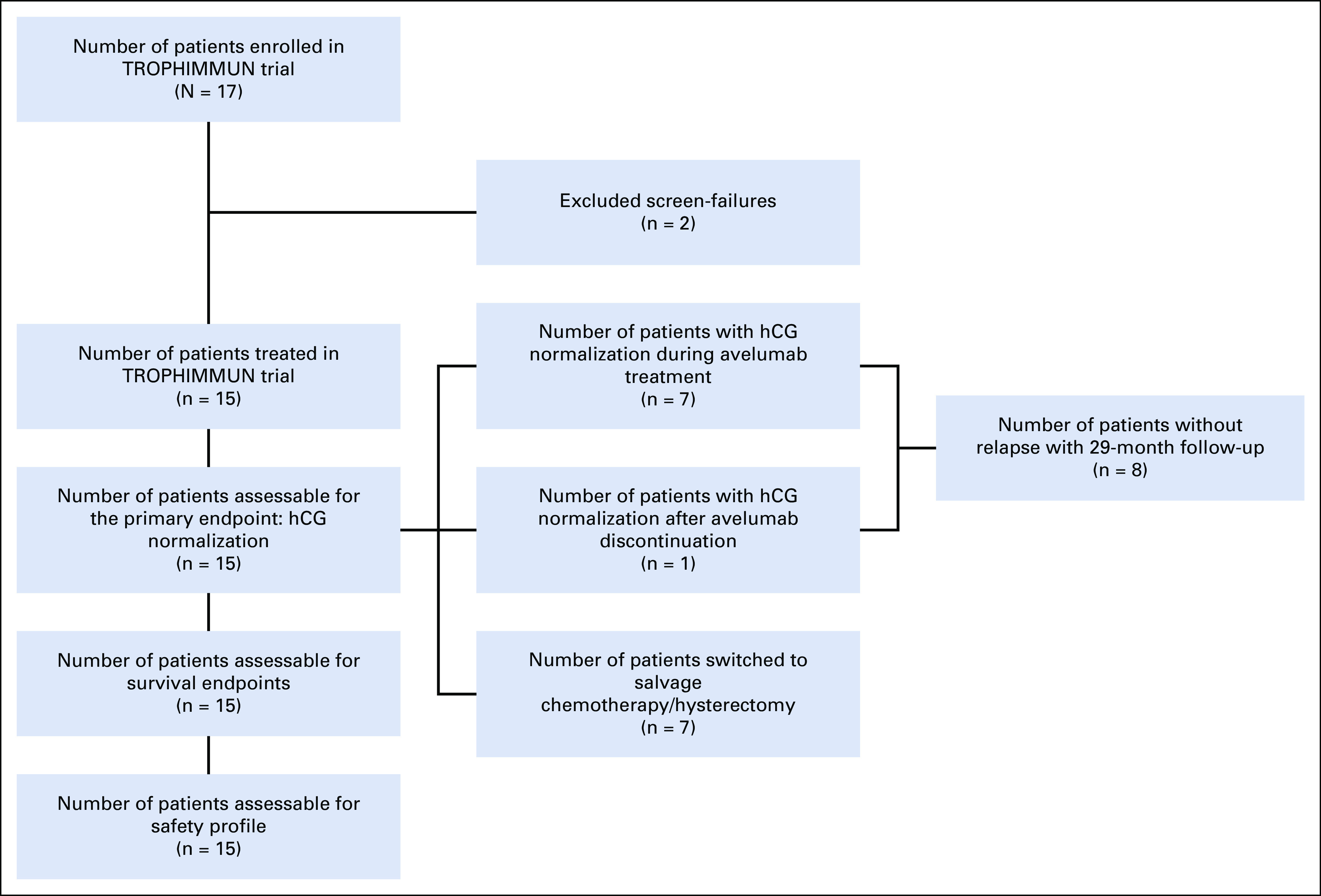
In this phase II multicenter trial (ClinicalTrials.gov identifier: NCT03135769), women with GTT who experienced disease progression after single-agent chemotherapy received avelumab 10 mg/kg intravenously every 2 weeks until human chorionic gonadotropin (hCG) normalization, followed by 3 consolidation cycles. Rate of hCG normalization was the primary endpoint (2-step Simon design).
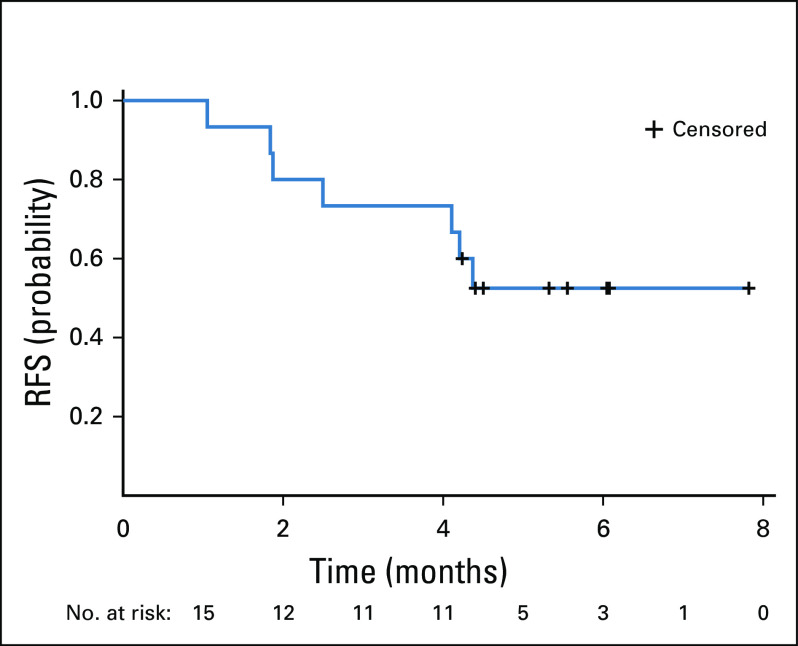
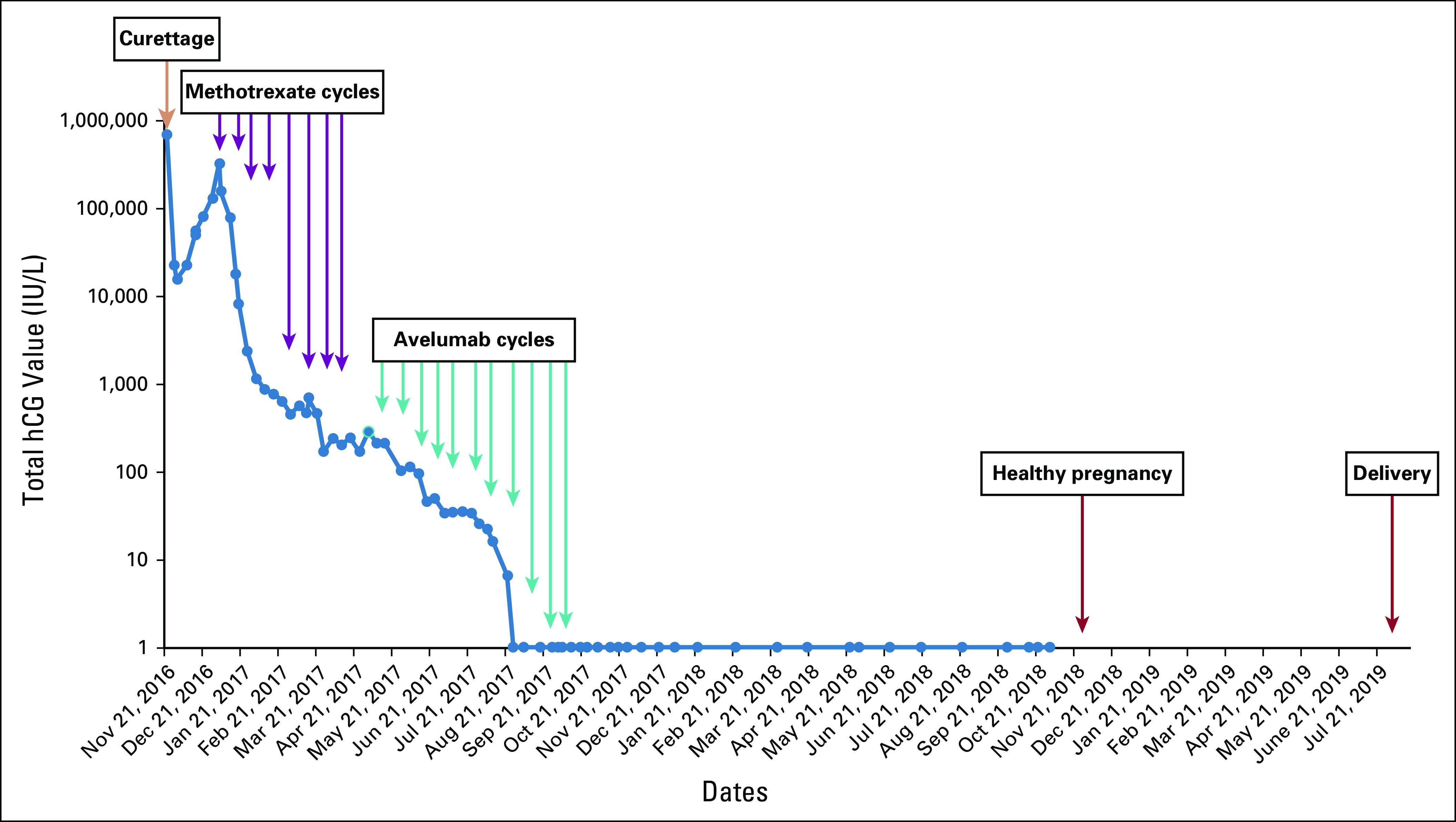
Between December 2016 and September 2018, 15 patients were treated. Median age was 34 years; disease stage was I or III in 53.3% and 46.7% of women, respectively; and International Federation of Gynecology and Obstetrics (FIGO) score was 0-4 in 33.3%, 5-6 in 46.7%, and ≥ 7 in 20% of patients. Prior treatment included methotrexate (100%) and actinomycin D (7%). Median follow-up was 25 months, and median number of avelumab cycles was 8 (range, 2-11). Grade 1-2 treatment-related adverse events occurred in 93% of patients, most commonly (≥ 25%) fatigue (33.3%), nausea/vomiting (33.3%), and infusion-related reaction (26.7%). One patient had grade 3 uterine bleeding (treatment unrelated). Eight patients (53.3%) had hCG normalization after a median of 9 avelumab cycles; none subsequently relapsed. Probability of normalization was not associated with disease stage, FIGO score, or baseline hCG. One patient subsequently had a healthy pregnancy. In avelumab-resistant patients (46.7%), hCG was normalized with actinomycin D (42.3%) or combination chemotherapy/surgery (57.1%).
In patients with single-agent chemotherapy-resistant GTT, avelumab had a favorable safety profile and cured approximately 50% of patients. Avelumab could be a new therapeutic option, particularly in patients who would otherwise receive combination chemotherapy.
对单一药物化疗耐药的妊娠滋养细胞肿瘤(GTT)患者接受替代化疗方案,这些方案虽然有效,但会引起相当大的毒性。所有 GTT 亚型均表达程序性死亡配体 1(PD-L1),自然杀伤(NK)细胞参与滋养细胞免疫监视。Avelumab(抗 PD-L1)诱导 NK 细胞介导的细胞毒性。TROPHIMMUN 试验评估了avelumab 在化疗耐药性 GTT 女性中的应用。
这是一项多中心二期临床试验(ClinicalTrials.gov 标识符:NCT03135769),在接受单药化疗后疾病进展的 GTT 患者中,给予avelumab 10mg/kg,每 2 周静脉注射一次,直至人绒毛膜促性腺激素(hCG)正常化,然后进行 3 个巩固周期。hCG 正常化率是主要终点(2 步 Simon 设计)。
2016 年 12 月至 2018 年 9 月,共治疗了 15 名患者。中位年龄为 34 岁;53.3%和 46.7%的患者疾病分期分别为 I 期或 III 期;国际妇产科联合会(FIGO)评分 0-4 分占 33.3%,5-6 分占 46.7%,≥ 7 分占 20%。既往治疗包括甲氨蝶呤(100%)和放线菌素 D(7%)。中位随访时间为 25 个月,avelumab 周期中位数为 8 个(范围 2-11 个)。93%的患者出现 1-2 级治疗相关不良事件,最常见的(≥ 25%)为疲劳(33.3%)、恶心/呕吐(33.3%)和输注相关反应(26.7%)。1 例患者发生 3 级子宫出血(与治疗无关)。中位 avelumab 周期 9 个后,8 名患者(53.3%)hCG 正常化;无患者随后复发。hCG 正常化的概率与疾病分期、FIGO 评分或基线 hCG 无关。1 例患者随后怀孕并分娩健康婴儿。在 avelumab 耐药患者(46.7%)中,放线菌素 D(42.3%)或联合化疗/手术(57.1%)使 hCG 正常化。
在单一药物化疗耐药的 GTT 患者中,avelumab 具有良好的安全性,约 50%的患者获得治愈。Avelumab 可能是一种新的治疗选择,特别是对那些需要接受联合化疗的患者。