Nephrology Department, Peking Union Medical College Hospital, Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing, China.
Pharmacy Department, Peking Union Medical College Hospital, Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing, China.
Cancer Med. 2020 Sep;9(18):6576-6585. doi: 10.1002/cam4.3198. Epub 2020 Jul 27.
Although kidney impairments have been reported following immune checkpoint inhibitors (ICIs) in clinical studies, there are few pharmacoepidemiology studies to compare the occurrences, clinical features, and prognosis of renal adverse effects.
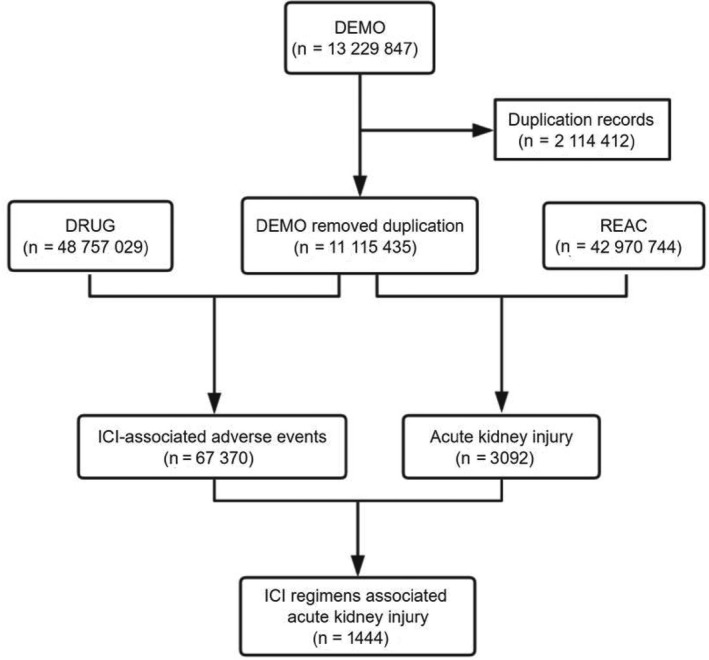
Disproportionality and Bayesian analysis were used in data mining to screen the suspected renal adverse effects after the administration of different ICIs, based on FDA's Adverse Event Reporting System (FAERS) from January 2004 to September 2019. The time to onset, fatality and hospitalization rates of renal adverse effects were also investigated.
We identified 1444 reports of renal adverse effects. Affected patients tended to be older than 65 years (52.7%). Renal effects were most commonly reported in nivolumab monotherapy (33.24%). Atezolizumab appeared the strongest association among six ICI monotherapies, based on the highest reporting odds ratio (ROR = 144.38, two-sided 95% CI = 123.08 -169.37), proportional reporting ratio (PRR = 139.13, χ = 21 425.38), and empirical Bayes geometric mean (EBGM = 131.75, one-sided 95% CI = 115.28). The combination treatments showed higher RORs, PRRs, and EBGMs, compared with either nivolumab or pembrolizumab monotherapy. The median onset time of renal adverse effects was 48 (interquartile range [IQR] 18.75-121.25) days after the monotherapies of ICI regimens. Patients treated with the combination of nivolumab plus ipilimumab were younger than receivers in nivolumab monotherapy (63.81 ± 12.03 vs 66.39 ± 11.53, P = .004); The fatality rate of renal adverse effects appeared lower in the combination group, compared to nivolumab monotherapy (18.53% vs 27.50%, P = .004). The top hospitalization rates due to renal effects occurred in patients with combination therapies.
Based on the FAERS database, we profiled renal adverse effects after various ICIs with real-world data in occurrences, clinical characteristics, and prognosis. Renal effects should be tightly monitored, especially within the first several months after ICIs administration. Particular concern should be paid for patients with a tendency for kidney impairments, such as old age.
虽然在临床研究中已经报道了免疫检查点抑制剂(ICI)治疗后出现的肾脏损伤,但很少有药物流行病学研究来比较肾脏不良反应的发生、临床特征和预后。
基于 FDA 的不良事件报告系统(FAERS),我们使用数据挖掘中的比例失衡和贝叶斯分析来筛选不同 ICI 治疗后疑似肾脏不良反应的病例,该系统的数据时间跨度为 2004 年 1 月至 2019 年 9 月。我们还调查了肾脏不良反应的发病时间、死亡率和住院率。
我们共鉴定出 1444 例肾脏不良反应报告。受影响的患者年龄往往大于 65 岁(52.7%)。在纳武单抗单药治疗中最常报告肾脏效应(33.24%)。在 6 种 ICI 单药治疗中,阿特珠单抗的报告比值比(ROR)最高(ROR=144.38,双侧 95%置信区间[CI]为 123.08-169.37),比例报告比(PRR)最高(PRR=139.13,χ 2=21425.38),经验贝叶斯几何均值(EBGM)最高(EBGM=131.75,单侧 95%CI 为 115.28)。与纳武单抗或帕博利珠单抗单药治疗相比,联合治疗的 ROR、PRR 和 EBGM 更高。ICI 方案单药治疗后,肾脏不良反应的中位发病时间为 48(四分位距[IQR] 18.75-121.25)天。与纳武单抗单药治疗组相比,接受纳武单抗联合伊匹单抗治疗的患者年龄更小(63.81±12.03 岁比 66.39±11.53 岁,P=.004);与纳武单抗单药治疗组相比,联合治疗组的肾脏不良反应死亡率较低(18.53%比 27.50%,P=.004)。因肾脏不良反应而住院的患者中,联合治疗组的比例最高。
基于 FAERS 数据库,我们使用真实世界数据描述了不同 ICI 治疗后的肾脏不良反应的发生、临床特征和预后。应密切监测肾脏不良反应,尤其是在 ICI 治疗后最初几个月内。对于有肾脏损伤倾向的患者,如老年患者,应特别注意。