CIC-1431 INSERM, CHU Besançon, Université de Franche-Comté, Besançon, France.
UMR1098 RIGHT, Université Bourgogne Franche-Comté, EFS, INSERM, Besançon, France.
PLoS One. 2020 Jul 28;15(7):e0236698. doi: 10.1371/journal.pone.0236698. eCollection 2020.
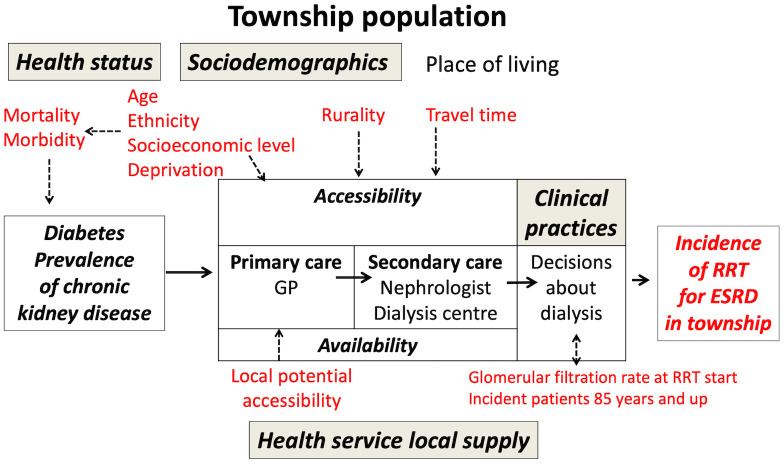
The strong geographic variations in the incidence rates of renal replacement therapy (RRT) for end-stage renal disease are not solely related to variations in the population's needs, such as the prevalence of diabetes or the deprivation level. Inequitable geographic access to health services has been involved in different countries but never in France, a country with a generous supply of health services and where the effect of the variability of medical practices was highlighted in an analysis conducted at the geographic scale of districts. Our ecological study, performed at the finer scale of townships in a French area of 8,370,616 inhabitants, investigated the association between RRT incidence rates, socioeconomic environment and geographic accessibility to healthcare while adjusting for morbidity level and medical practice patterns.
Using data from the Renal Epidemiology and Information Network registry, we estimated age-adjusted RRT incidence rates during 2010-2014 for the 282 townships of the area. A hierarchical Bayesian Poisson model was used to examine the association between incidence rates and 18 contextual variables describing population health status, socioeconomic level and health services characteristics. Relative risks (RRs) and 95% credible intervals (95% CrIs) for each variable were estimated for a 1-SD increase in incidence rate.
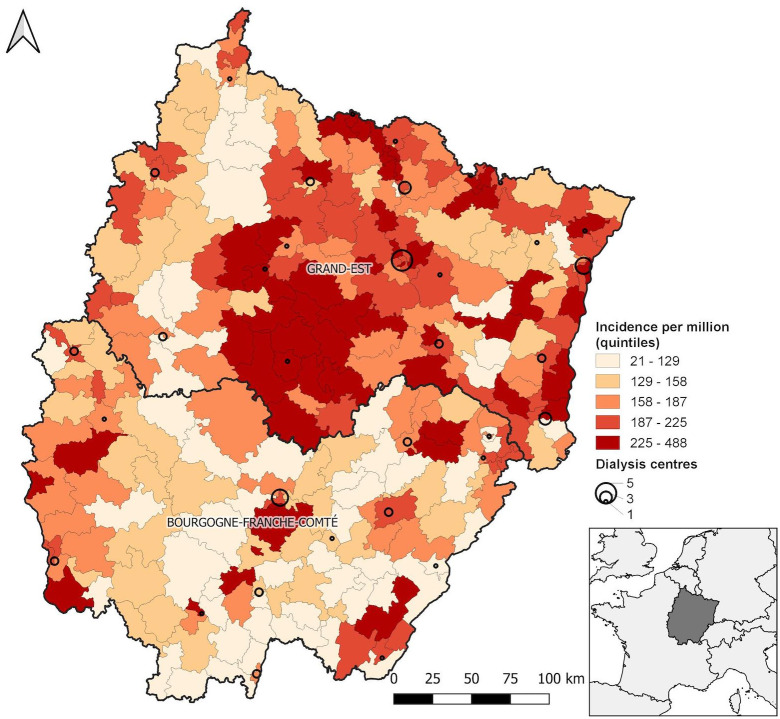
During 2010-2014, 6,835 new patients ≥18 years old (4231 men, 2604 women) living in the study area started RRT; the RRT incidence rates by townships ranged from 21 to 499 per million inhabitants. In multivariate analysis, rates were related to the prevalence of diabetes [RR (95% CrI): 1.05 (1.04-1.11)], the median estimated glomerular filtration rate at dialysis initiation [1.14 (1.08-1.20)], and the proportion of incident patients ≥ 85 years old [1.08 (1.03-1.14)]. After adjusting for these factors, rates in townships increased with increasing French deprivation index [1.05 (1.01-1.08)] and decreased with increasing mean travel time to reach the closest nephrologist [0.92 (0.89-0.95]).
These data confirm the influence of deprivation level, the prevalence of diabetes and medical practices on RRT incidence rates across a large French area. For the first time, an association was found with the distance to nephrology services. These data suggest possible inequitable geographic access to RRT within the French health system.
终末期肾病的肾脏替代治疗(RRT)发生率存在较强的地域差异,这不仅与人口需求的变化(如糖尿病的流行程度或贫困水平)有关。在不同国家,医疗服务的地理分布不均一直是一个问题,但在法国从未出现过这种情况,法国拥有丰富的医疗服务资源,而且在对地区范围内的医疗实践差异进行分析时,已经强调了这种医疗服务的地理分布不均。本生态研究在法国一个拥有 8370616 名居民的地区,以乡镇为更细的尺度,调查了 RRT 发生率与社会经济环境和医疗服务地理可及性之间的关系,同时调整了发病率水平和医疗实践模式的影响。
我们利用肾脏流行病学和信息网络登记处的数据,估算了 2010 年至 2014 年该地区 282 个乡镇的年龄调整后 RRT 发生率。使用分层贝叶斯泊松模型,研究了发生率与描述人口健康状况、社会经济水平和卫生服务特征的 18 个背景变量之间的关系。对于每个变量,我们都根据发生率的 1-SD 增加来估计相对风险(RR)和 95%可信区间(95% CrI)。
在 2010 年至 2014 年期间,该地区 282 个乡镇中共有 6835 名年龄≥18 岁的新患者(4231 名男性,2604 名女性)开始接受 RRT;乡镇 RRT 发生率范围为 21 至 499/百万居民。在多变量分析中,发生率与糖尿病的流行程度有关[RR(95% CrI):1.05(1.04-1.11)]、透析开始时估计的肾小球滤过率中位数[1.14(1.08-1.20)]和≥85 岁新发病例的比例[1.08(1.03-1.14)]。在调整了这些因素后,乡镇的 RRT 发生率随着法国贫困指数的增加而增加[1.05(1.01-1.08)],随着到达最近的肾病医生的平均旅行时间的增加而减少[0.92(0.89-0.95)]。
这些数据证实了剥夺程度、糖尿病的流行程度和医疗实践对法国一个大型地区 RRT 发生率的影响。首次发现与肾病服务的距离有关。这些数据表明,在法国卫生系统内,RRT 的地理分布可能存在不公平现象。