Shnaydman Ilya, Abdelhamid Mohamed O, Kaufman Joyce, Lieberman Howard, Ruiz Gabriel
Department of Surgery, Ryder Trauma Center, 1800 NW 10th Ave, Miami, FL, 33136, USA.
J Cardiothorac Surg. 2020 Jul 28;15(1):193. doi: 10.1186/s13019-020-01240-w.
Left ventricular assist devices (LVAD) are placed for patients with advanced heart failure or cardiogenic shock as destination therapy or as a bridge to cardiac transplantation. Significant complications associated with LVAD placement include bleeding, infection, pump thrombosis, right heart failure, device malfunction and stroke. The case below illustrates inadvertent intraperitoneal driveline placement causing colonic perforation and the subsequent management.
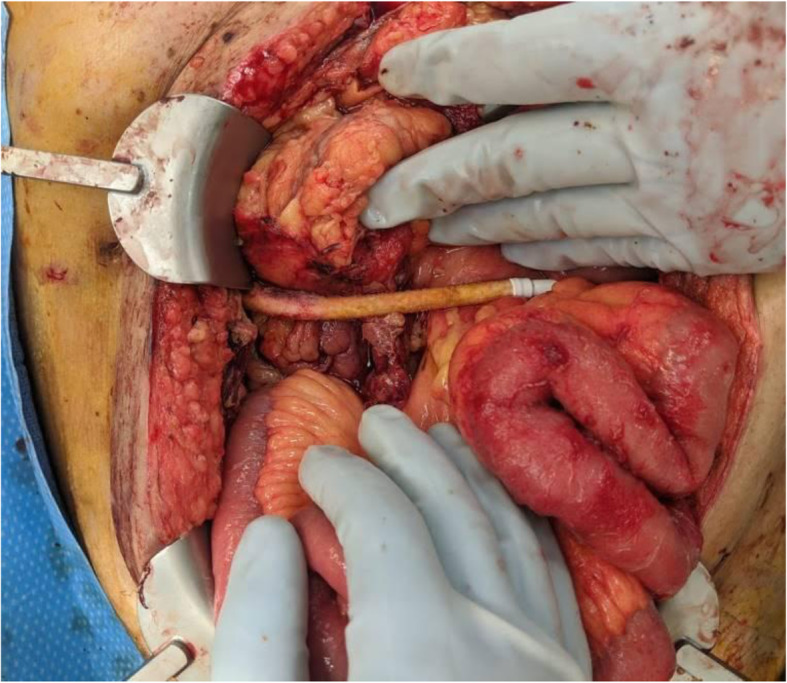
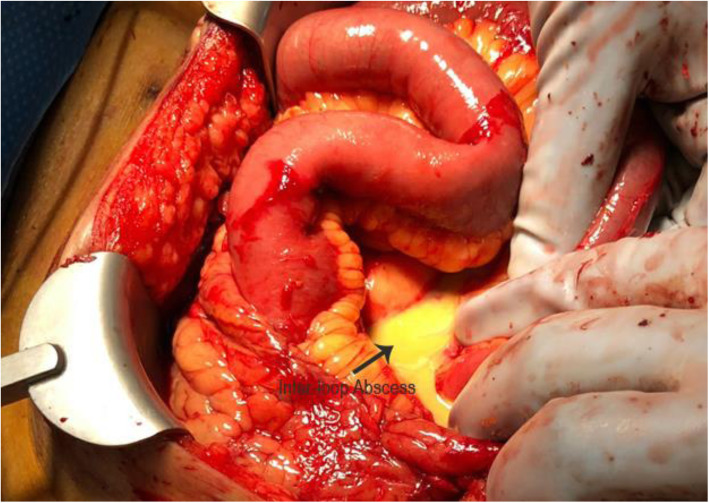
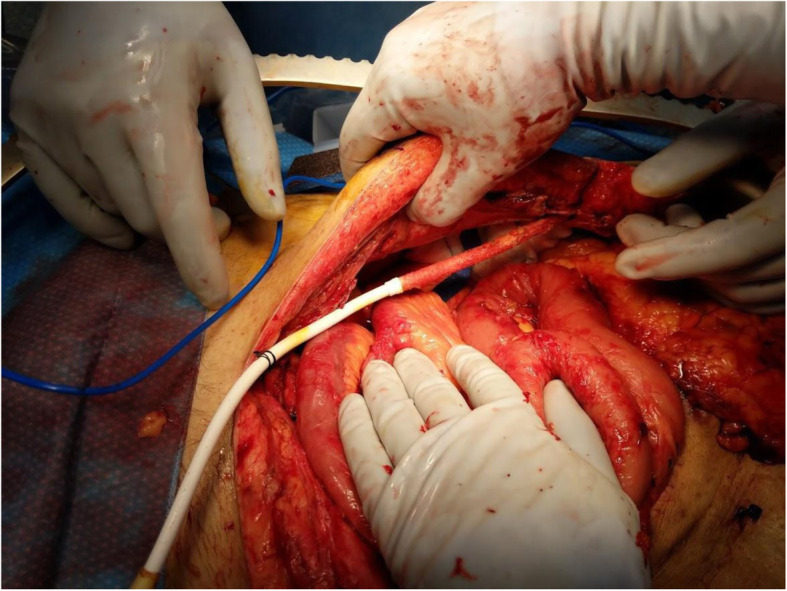
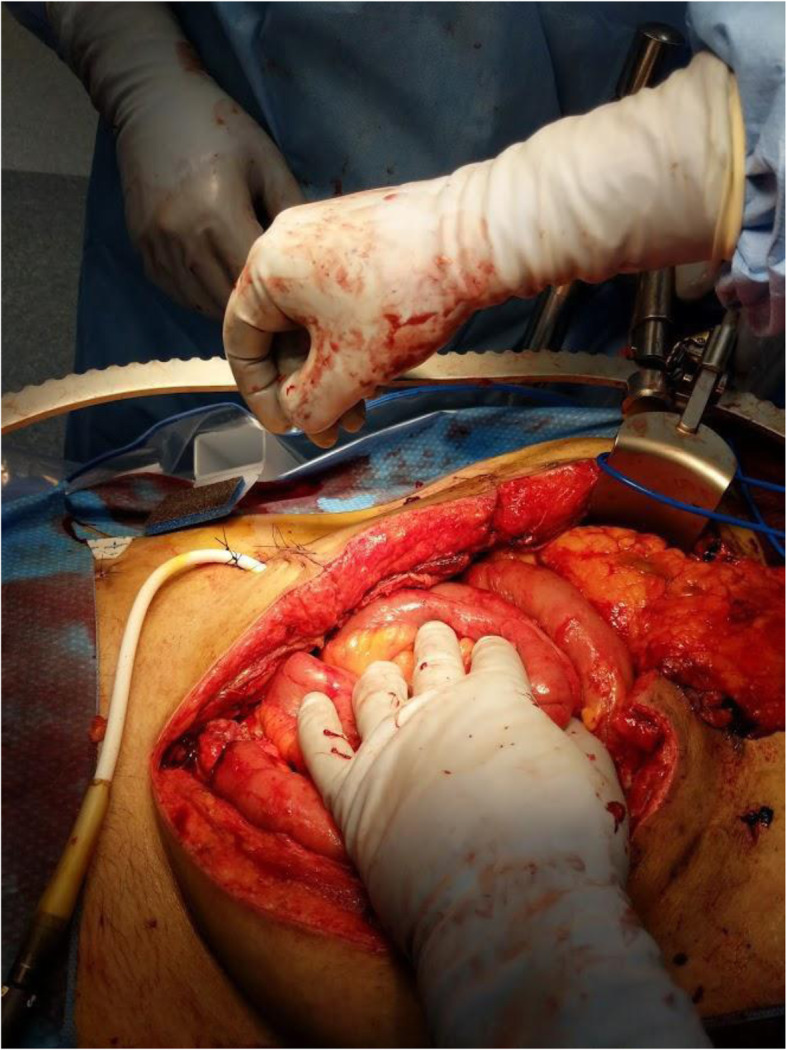
A 54 year old male with a history of Wolff-Parkinson-White syndrome resulting in multiple readmissions for heart failure, ultimately required placement of a left ventricular assist device (LVAD). Several weeks later, he was found to have stool draining from the driveline site. The patient was taken to the operating room for limited exploration by the Cardiothoracic Surgery team and a bowel injury was identified and repaired. Three days after this repair, stool was once again leaking from the driveline site, requiring re-exploration by the Acute Care Surgery team. Intraoperatively, the prior repair was found to be leaking and multiple intra-abdominal abscesses were discovered. The transverse colon was resected and left in discontinuity. On a planned second look operation, the LVAD driveline was relocated to be extra-peritoneal and a colostomy was formed.
This case demonstrates the importance of early recognition and involvement of an Acute Care Surgeon in the management of this complex problem. Appropriate treatment involves a complete exploration, source control, driveline relocation and possible fecal diversion. Although the incidence of this complication is low, it must be considered in the differential in a septic LVAD patient.
左心室辅助装置(LVAD)用于晚期心力衰竭或心源性休克患者,作为终末期治疗或心脏移植的桥梁。与LVAD植入相关的重大并发症包括出血、感染、泵血栓形成、右心衰竭、装置故障和中风。以下病例说明了无意中将驱动线置于腹腔内导致结肠穿孔及后续处理情况。
一名54岁男性,有预激综合征病史,因心力衰竭多次入院,最终需要植入左心室辅助装置(LVAD)。几周后,发现有粪便从驱动线部位流出。患者被心胸外科团队送往手术室进行有限的探查,发现并修复了肠道损伤。此次修复三天后,粪便再次从驱动线部位渗漏,需要急性护理外科团队再次探查。术中发现先前的修复处渗漏,并发现多个腹腔内脓肿。横结肠被切除并保持间断。在计划的二次探查手术中,LVAD驱动线被重新放置在腹膜外,并形成了结肠造口术。
该病例表明了急性护理外科医生早期识别并参与处理这一复杂问题的重要性。恰当的治疗包括全面探查、源头控制、驱动线重新定位以及可能的粪便转流。尽管这种并发症的发生率较低,但在LVAD感染患者的鉴别诊断中必须予以考虑。