Dallas Diabetes Research Center at Medical City, Dallas, Texas, USA.
Department of Medicine, Clinical University Hospital, University of Valencia, Valencia, Spain.
Diabetes Obes Metab. 2020 Dec;22(12):2295-2304. doi: 10.1111/dom.14154. Epub 2020 Sep 2.
To assess the impact of the timing of initiating both basal insulin and glucagon-like peptide-1 receptor agonists (GLP-1 RAs) on reaching glycaemic control targets over 6 and 12 months in people with type 2 diabetes (T2D) uncontrolled on oral antihyperglycaemic drugs with an HbA1c of 9% or higher.
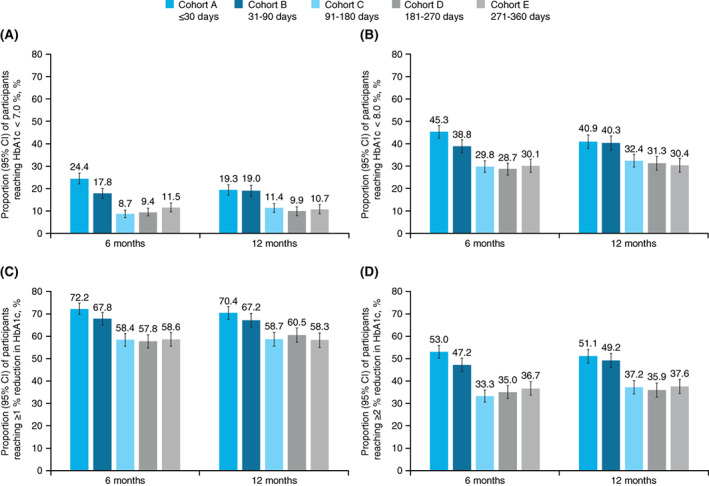
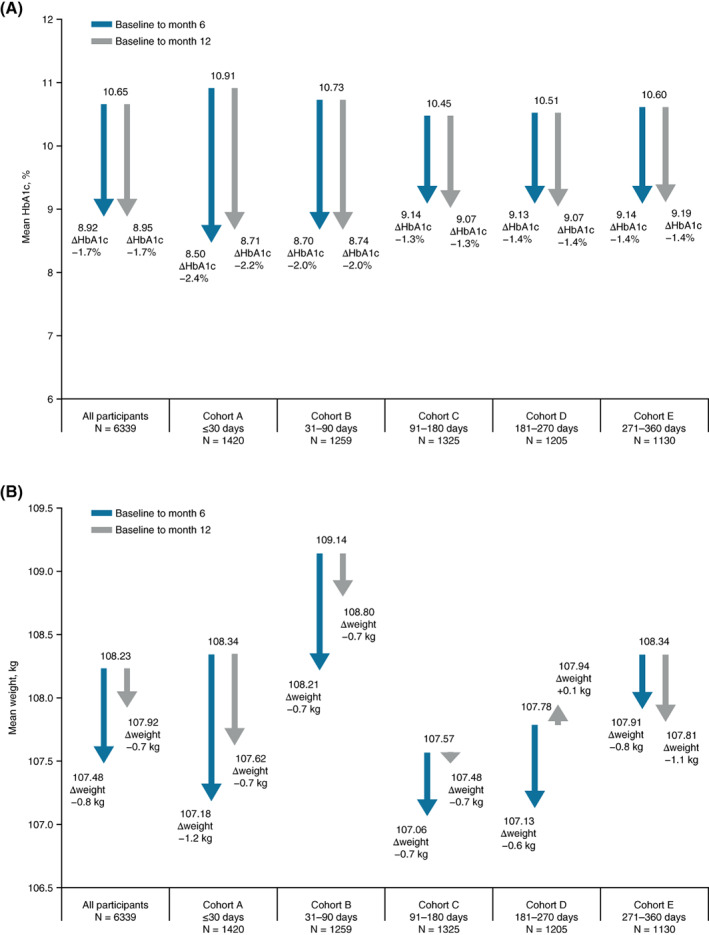
This retrospective cohort study assessed the impact of the timing of initiating both basal insulin and GLP-1 RA therapies on reaching glycaemic targets (HbA1c < 7% and <8%, and ≥1% and ≥2% HbA1c reduction) over 12 months in people with markedly uncontrolled T2D (HbA1c ≥ 9%) on oral antihyperglycaemic drugs identified on the Optum Humedica database (electronic medical records; 1 January 2011 to 30 June 2017). Study cohorts were defined by the days between initiating each injectable: cohort A, 30 days or less (simultaneous initiation) and cohorts B, 31-90, C, 91-180, D, 181-270 and E, 271-360 days (sequential initiation).
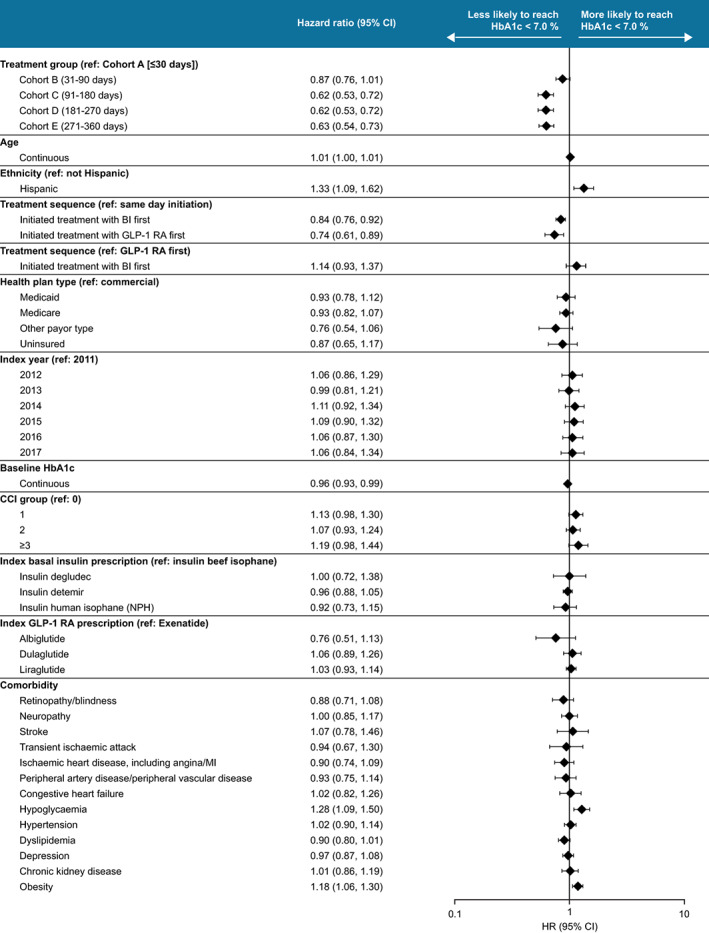
Cohort A had the best glycaemic outcomes at 6 and 12 months for all four endpoints, followed by cohort B. The likelihood of achieving an HbA1c of less than 7% did not significantly differ between cohorts A and B (hazard ratio [95% confidence interval]: 0.87 [0.76-1.01]); cohorts C, D and E were significantly less likely to achieve an HbA1c of less than 7% than cohort A (0.62 [0.53-0.72]; 0.62 [0.53-0.72]; 0.63 [0.54-0.73]).
In people with uncontrolled T2D requiring treatment with a GLP-1 RA and basal insulin, greater improvements in glycaemic control were observed when both therapies were initiated within close proximity of one another (≤90 days) compared with initiation 91-360 days apart.
评估在口服降糖药物控制不佳(HbA1c >9%)的 2 型糖尿病(T2D)患者中,起始基础胰岛素和胰高血糖素样肽-1 受体激动剂(GLP-1 RA)的时间对 6 个月和 12 个月时达到血糖控制目标的影响。
本回顾性队列研究评估了在 Optum Humedica 数据库(电子病历;2011 年 1 月 1 日至 2017 年 6 月 30 日)中,起始基础胰岛素和 GLP-1 RA 治疗的时间对糖化目标(HbA1c<7%和<8%,以及≥1%和≥2%的 HbA1c 降低)的影响,研究人群为口服降糖药物控制不佳的 T2D 患者(HbA1c≥9%)。研究队列根据起始每种注射药物的天数定义:队列 A,30 天或更短(同时起始),队列 B,31-90 天,队列 C,91-180 天,队列 D,181-270 天,队列 E,271-360 天(序贯起始)。
在所有四个终点中,6 个月和 12 个月时,A 队列的血糖控制效果最佳,其次是 B 队列。与 A 队列相比,A 和 B 队列(风险比[95%置信区间]:0.87[0.76-1.01])达到 HbA1c<7%的可能性无显著差异;与 A 队列相比,C、D 和 E 队列达到 HbA1c<7%的可能性显著降低(0.62[0.53-0.72];0.62[0.53-0.72];0.63[0.54-0.73])。
在需要 GLP-1 RA 和基础胰岛素治疗的血糖控制不佳的 T2D 患者中,与起始时间相隔 91-360 天相比,两种治疗方法起始时间接近(≤90 天)时,血糖控制的改善更显著。