Peng Xuejun Victor, Ayyagari Rajeev, Lubwama Robert, Shi Lizheng, Price-Haywood Eboni G, Hollander Priscilla, Fonseca Vivian
Sanofi US, Inc., 55 Corporate Dr., Bridgewater, NJ, USA.
Analysis Group, Inc., 111 Huntington Ave., 14th Floor, Boston, MA, USA.
Diabetes Ther. 2020 Apr;11(4):995-1005. doi: 10.1007/s13300-020-00783-4. Epub 2020 Feb 28.
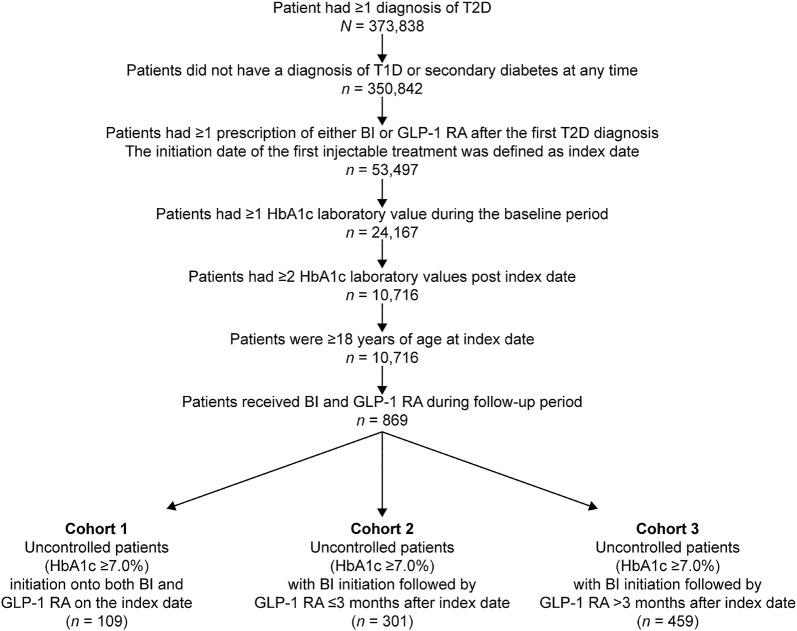
When and how to intensify treatment in patients with type 2 diabetes (T2D) not achieving glycated hemoglobin (HbA1c) targets with oral antidiabetic drugs (OADs) in clinical practice remains a matter of clinical preference. This pilot study was conducted using the retrospective observational data from such patients to evaluate the impact on HbA1c of three treatment sequences: simultaneous initiation of basal insulin (BI) and a glucagon-like peptide-1 receptor agonist (GLP-1 RA; Cohort 1); BI followed by GLP-1 RA initiation within a 90-day timeframe (Cohort 2); or BI followed by GLP-1 RA initiation beyond 90 days (Cohort 3).
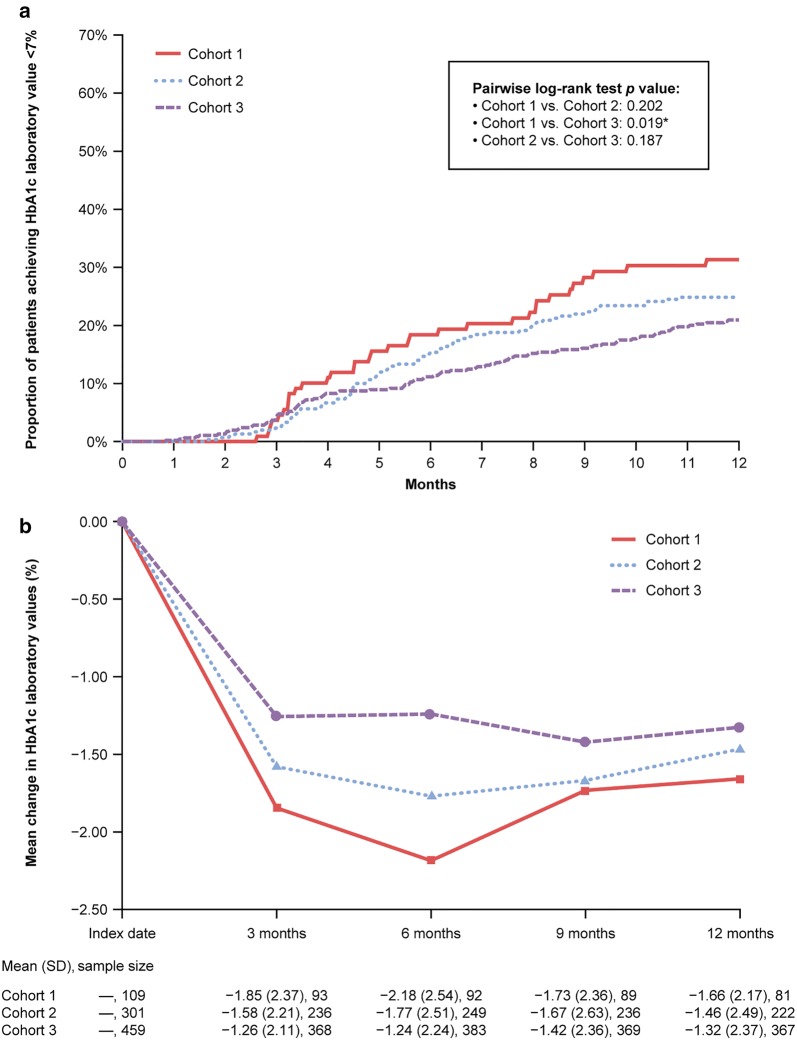
Data from the regional US electronic medical records database, Research Action for Health Network (REACHnet), were extracted for all patients with T2D aged ≥ 18 years who had encounter dates between January 2011 and August 2017 and ≥ 1 HbA1c laboratory value(s) < 90 days before BI initiation and ≥ 2 HbA1c laboratory values within 1 year after BI initiation and who met the inclusion criteria for GLP-1 RA initiation set for Cohorts 1, 2, or 3. The primary endpoints were the proportion of patients achieving HbA1c < 7.0%, which was estimated via Kaplan-Meier analysis, and change in HbA1c within 12 months.
Overall, 869 patients were analyzed, of whom 109 were in Cohort 1, 301 in Cohort 2, and 459 in Cohort 3. Baseline HbA1c was 10.3 ± 2.1, 10.3 ± 2.0, and 10.2 ± 2.1% for these three cohorts, respectively. Statistically significantly more patients in Cohort 1 than in Cohort 3 achieved HbA1c < 7.0% (33.4 vs. 20.9%, respectively; p = 0.0186). Mean observed reductions in HbA1c at 12 months were - 1.7% (Cohort 1), - 1.5% (Cohort 2), and - 1.3% (Cohort 3).
Simultaneous initiation of BI and GLP-1 RA achieves glycemic control more effectively than sequential initiation of BI with GLP-1 RA added beyond 90 days.
在临床实践中,对于使用口服降糖药(OADs)未达到糖化血红蛋白(HbA1c)目标的2型糖尿病(T2D)患者,何时以及如何强化治疗仍是临床偏好问题。本试点研究利用这些患者的回顾性观察数据,评估三种治疗顺序对HbA1c的影响:同时起始基础胰岛素(BI)和胰高血糖素样肽-1受体激动剂(GLP-1 RA;队列1);在90天内先起始BI,随后起始GLP-1 RA(队列2);或在90天后先起始BI,随后起始GLP-1 RA(队列3)。
从美国区域电子病历数据库“健康网络研究行动”(REACHnet)中提取数据,纳入所有年龄≥18岁的T2D患者,这些患者在2011年1月至2017年8月期间有就诊记录,在起始BI前<90天有≥1次HbA1c实验室检测值,在起始BI后1年内有≥2次HbA1c实验室检测值,且符合队列1、2或3设定的GLP-1 RA起始纳入标准。主要终点为达到HbA1c<7.0%的患者比例(通过Kaplan-Meier分析估算)以及12个月内HbA1c的变化。
总体共分析了869例患者,其中队列1有109例,队列2有301例,队列3有459例。这三个队列的基线HbA1c分别为10.3±2.1%、10.3±2.0%和10.2±2.1%。队列1中达到HbA1c<7.0%的患者在统计学上显著多于队列3(分别为33.4%和20.9%;p=0.0186)。12个月时观察到的HbA1c平均降低值在队列1中为-1.7%,队列2中为-1.5%,队列3中为-1.3%。
同时起始BI和GLP-1 RA比在90天后添加GLP-1 RA的顺序起始BI能更有效地实现血糖控制。