Department of Endocrine and Metabolic Diseases, Istituto Auxologico Italiano, Istituto Di Ricovero e Cura a Carattere Scientifico (IRCCS), Milan, Italy.
Department of Pathophysiology and Transplantation, University of Milan, Milan, Italy.
Front Endocrinol (Lausanne). 2020 Jul 7;11:432. doi: 10.3389/fendo.2020.00432. eCollection 2020.
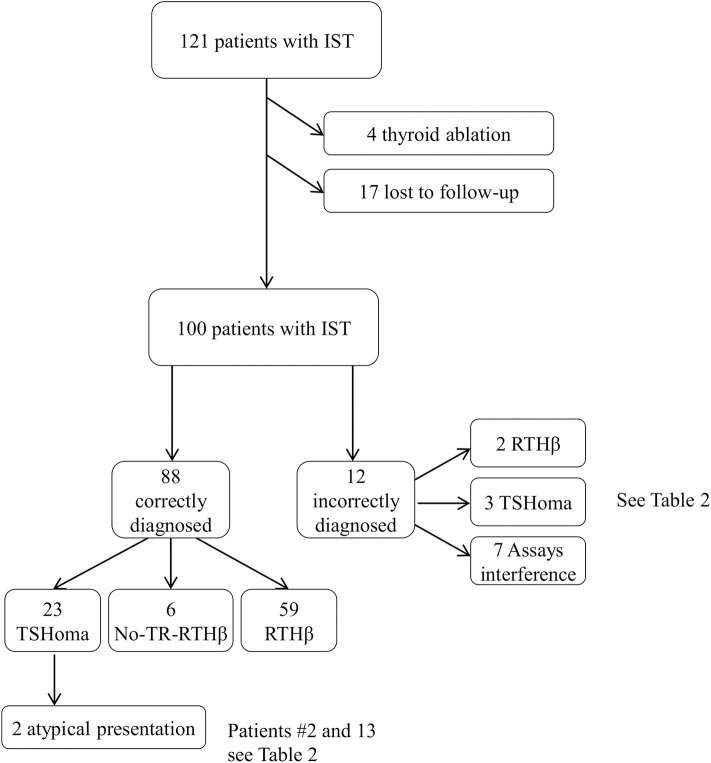
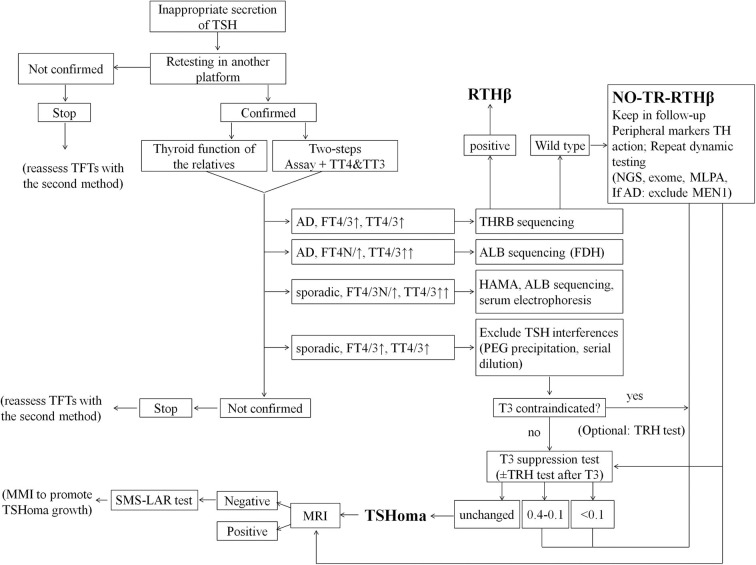
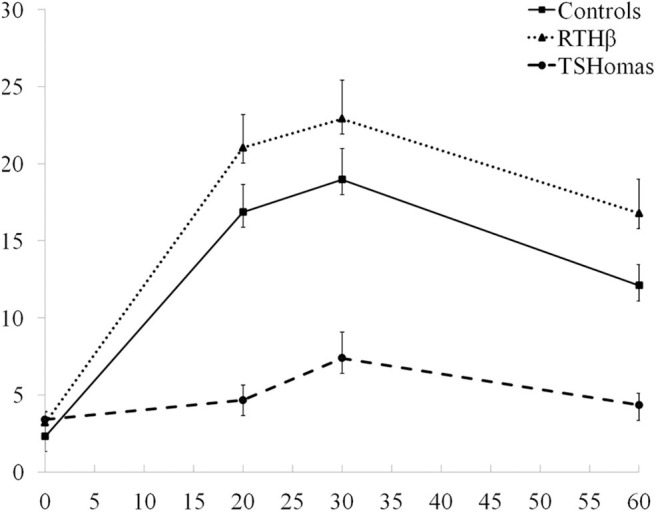
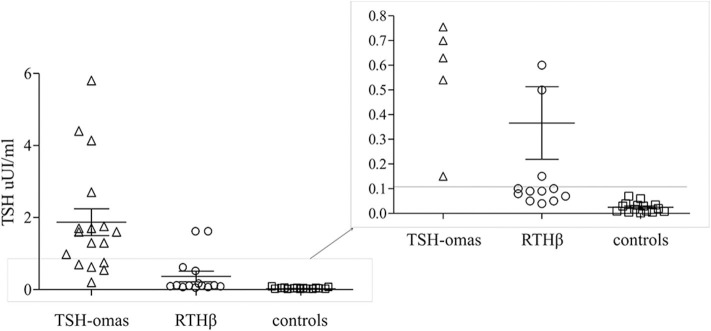
Discrepant thyroid function tests (TFTs) are typical of inappropriate secretion of TSH (IST), a rare entity encompassing TSH-secreting adenomas (TSHoma) and Resistance to Thyroid Hormone (RTHβ) due to mutations. The differential diagnosis remains a clinical challenge in most of the cases. The objective of this study was to share our experience with patients presenting with discrepant TFTs outlining the main pitfalls in the differential diagnosis. medical records of 100 subjects with discrepant TFTs referred to Thyroid Endocrine Centers at the University of Milan were analyzed, retrospectively. Patients were studied by dynamic testing (TRH test, T3-suppression test, or a short course of long-acting somatostatin analog, when appropriate), sequencing, and pituitary imaging. 88 patients were correctly diagnosed as RTHβ with ( = 59; 16 men, 43 women) or without variants ( = 6; 2 men, 4 female) or TSHoma ( = 23; 9 men, 14 women). We identified 14 representative subjects with an atypical presentation or who were misdiagnosed. Seven patients, with spurious hyperthyroxinemia due to assays interference were erroneously classified as RTHβ ( = 4) or TSHoma ( = 3). Three patients with genuine TSHomas were classified as laboratory artifact ( = 2) or RTHβ ( = 1). Two TSHomas presented atypically due to coexistent primary thyroid diseases. In one RTHβ a drug-induced thyroid dysfunction was primarily assumed. These patients experienced a mean diagnostic delay of 26 ± 14 months. Analysis of the investigations which can differentiate between TSHoma and RTHβ showed highest accuracy for the T3-suppression test (100% specificity with a cut-off of TSH <0.11 μUI/ml). Pituitary MRI was negative in 6/26 TSHomas, while 11/45 RTHβ patients had small pituitary lesions, leading to unnecessary surgery in one case. Diagnostic delay and inappropriate treatments still occur in too many cases with discrepant TFTs suggestive of central hyperthyroidism. The insistent pitfalls lead to a significant waste of resources. We propose a revised flow-chart for the differential diagnosis.
甲状腺功能检测结果不一致(TFTs)是促甲状腺激素(TSH)分泌不当(IST)的典型表现,这是一种罕见的疾病实体,包括 TSH 分泌腺瘤(TSHoma)和由于突变导致的甲状腺激素抵抗(RTHβ)。在大多数情况下,鉴别诊断仍然是一个临床挑战。本研究的目的是分享我们在处理表现为 TFTs 不一致的患者方面的经验,概述鉴别诊断中的主要陷阱。
回顾性分析了米兰大学甲状腺内分泌中心 100 例 TFTs 不一致的患者的病历。对患者进行了动态检测(TRH 试验、T3 抑制试验或短期长效生长抑素类似物治疗,视情况而定)、测序和垂体成像。
88 例患者被正确诊断为 RTHβ,伴有(=59;16 名男性,43 名女性)或不伴有(=6;2 名男性,4 名女性)或 TSHoma(=23;9 名男性,14 名女性)。我们确定了 14 例具有非典型表现或误诊的有代表性的患者。由于检测干扰导致假性高甲状腺素血症,7 例患者被错误地归类为 RTHβ(=4)或 TSHoma(=3)。3 例真正的 TSHoma 被归类为实验室假象(=2)或 RTHβ(=1)。2 例 TSHoma 由于共存的原发性甲状腺疾病而表现异常。1 例 RTHβ 患者最初被认为是药物引起的甲状腺功能障碍。这些患者的平均诊断延迟为 26±14 个月。用于区分 TSHoma 和 RTHβ 的检查分析显示 T3 抑制试验的准确性最高(TSH<0.11μUI/ml 时的特异性为 100%)。在 26 例 TSHoma 中,垂体 MRI 为阴性,而在 45 例 RTHβ 患者中,11 例有小垂体病变,导致 1 例不必要的手术。
在表现为中枢性甲亢的 TFTs 不一致的情况下,诊断延迟和不适当的治疗仍然经常发生。顽固的陷阱导致了大量资源的浪费。我们提出了一个修订的鉴别诊断流程图。