Merchant Reshma Aziz, Hui Richard Jor Yeong, Kwek Sing Cheer, Sundram Meena, Tay Arthur, Jayasundram Jerome, Chen Matthew Zhixuan, Ng Shu Ee, Tan Li Feng, Morley John E
Division of Geriatric Medicine, Department of Medicine, National University Hospital, National University Health System, Singapore, Singapore.
Department of Medicine, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore.
Front Med (Lausanne). 2020 Jul 8;7:261. doi: 10.3389/fmed.2020.00261. eCollection 2020.
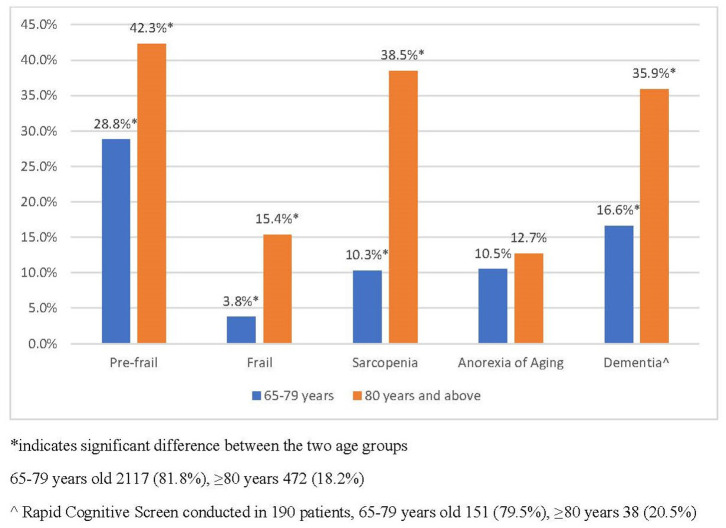
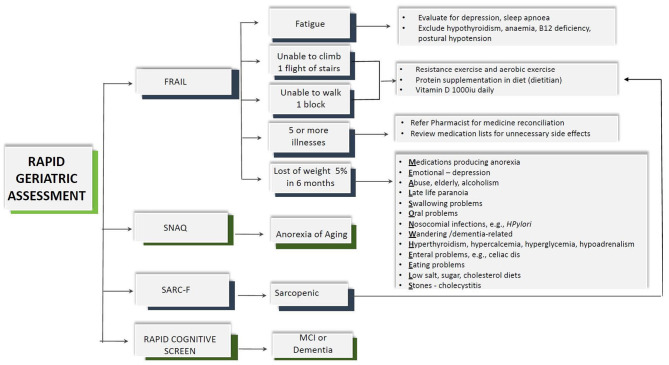
With the aging population and consequent increase in associated prevalence of frailty, dementia, and multimorbidity, primary care physicians will be overwhelmed with the complexity of the psychosocial and clinical presentation. Geriatric syndromes including frailty, sarcopenia, cognitive impairment, and anorexia of aging (AA) either in isolation or in combination are associated with an increased risk of adverse outcomes and if recognized early, and appropriately managed, will lead to decreased disability. Primary care practices are often located in residential settings and are in an ideal position to incorporate preventive screening and geriatric assessment with personalized management. However, primary care physicians lack the time, multidisciplinary resources, or skills to conduct geriatric assessment, and the limited number of geriatricians worldwide further complicates the matter. There is no one effective strategy to implement geriatric assessment in primary care which is rapid, cost-effective, and do not require geriatricians. Rapid Geriatric Assessment (RGA) takes <5 min to complete. It screens for frailty, sarcopenia, AA, and cognition with assisted management pathway without the need of a geriatrician. We developed RGA iPad application for screening with assisted management in two primary care practices and explored the feasibility and overall prevalence of frailty, sarcopenia, and AA. The assessment was conducted by trained nurses and coordinators. Among 2,589 older patients ≥65 years old, the prevalence of frailty was 5.9%, pre-frail 31.2%, and robust 62.9%. Fatigue was present in 17.8%, and among them, the prevalence of undiagnosed depression as assessed by the Patient Health Questionnaire (PHQ)-9 was 76.4% and 13.5% of total. The prevalence of sarcopenia was 15.4%, and 13.9% experienced at least one fall in the past year. AA was prevalent in 10.9%. The time taken to do the assessment with defined algorithm was on average 5 min or less per patient, and 96% managed to complete the assessment prior to seeing their doctor in the same session. The RGA app is a rapid and feasible tool to be used by any healthcare professional in primary care for identification of geriatric syndrome with assisted management.
随着人口老龄化以及随之而来的衰弱、痴呆和多种疾病并发的患病率增加,初级保健医生将被社会心理和临床表现的复杂性压得喘不过气来。包括衰弱、肌肉减少症、认知障碍和衰老性厌食(AA)在内的老年综合征,无论是单独出现还是合并出现,都与不良后果风险增加相关,如果能早期识别并得到适当管理,将减少残疾。初级保健机构通常位于居民区内,非常适合将预防性筛查和老年评估与个性化管理相结合。然而,初级保健医生缺乏进行老年评估的时间、多学科资源或技能,而且全球老年医学专家数量有限,使问题更加复杂。目前还没有一种有效的策略能在初级保健中实施快速、经济高效且无需老年医学专家的老年评估。快速老年评估(RGA)完成时间不到5分钟。它通过辅助管理途径筛查衰弱、肌肉减少症、AA和认知情况,无需老年医学专家参与。我们开发了RGA iPad应用程序,用于在两家初级保健机构进行辅助管理筛查,并探讨了衰弱、肌肉减少症和AA的可行性及总体患病率。评估由经过培训的护士和协调员进行。在2589名65岁及以上的老年患者中,衰弱患病率为5.9%,衰弱前期为31.2%,健康为62.9%。疲劳发生率为17.8%,其中根据患者健康问卷(PHQ)-9评估,未确诊抑郁症的患病率在疲劳患者中为76.4%,占总人数的13.5%。肌肉减少症患病率为15.4%,13.9%的患者在过去一年中至少跌倒过一次。AA患病率为10.9%。按照既定算法进行评估,平均每位患者用时5分钟或更短,96%的患者在同一次就诊看医生之前完成了评估。RGA应用程序是一种快速且可行的工具,可供初级保健中的任何医疗专业人员用于识别老年综合征并进行辅助管理。