School of Epidemiology and Public Health, University of Ottawa, 600 Peter Morand Crescent, Ottawa, Ontario, K1G 5Z3, Canada.
Jimma Zone Health Office, Jimma Zone, Oromia Region, Jimma, Ethiopia.
BMC Health Serv Res. 2020 Jul 31;20(1):703. doi: 10.1186/s12913-020-05572-0.
Analysis of disaggregated national data suggest uneven access to essential maternal healthcare services within countries. This is of concern as it hinders equitable progress in health outcomes. Mounting an effective response requires identification of subnational areas that may be lagging behind. This paper aims to explore spatial variation in maternal healthcare service use at health centre catchment, village and household levels. Spatial correlations of service use with household wealth and women's education levels were also assessed.
Using survey data from 3758 households enrolled in a cluster randomized trial geographical variation in the use of maternity waiting homes (MWH), antenatal care (ANC), delivery care and postnatal care (PNC) was investigated in three districts in Jimma Zone. Correlations of service use with education and wealth levels were also explored among 24 health centre catchment areas using choropleth maps. Global spatial autocorrelation was assessed using Moran's I. Cluster analyses were performed at village and household levels using Getis Ord Gi* and Kulldorf spatial scan statistics to identify cluster locations.
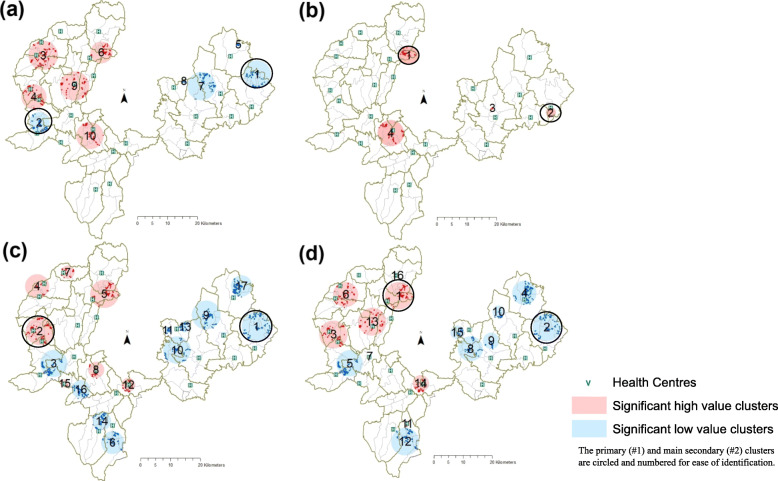
Significant global spatial autocorrelation was present in ANC use (Moran's I = 0.15, p value = 0.025), delivery care (Moran's I = 0.17, p value = 0.01) and PNC use (Moran's I = 0.31, p value < 0.01), but not MWH use (Moran's I = -0.005, p value = 0.94) suggesting clustering of villages with similarly high (hot spots) and/or low (cold spots) service use. Hot spots were detected in health centre catchments in Gomma district while Kersa district had cold spots. High poverty or low education catchments generally had low levels of service use, but there were exceptions. At village level, hot and cold spots were detected for ANC, delivery care and PNC use. Household-level analyses revealed a primary cluster of elevated MWH-use not detected previously. Further investigation of spatial heterogeneity is warranted.
Sub-national variation in maternal healthcare services exists in Jimma Zone. There was relatively higher poverty and lower education in areas where service use cold spots were identified. Re-directing resources to vulnerable sub-groups and locations lagging behind will be necessary to ensure equitable progress in maternal health.
对各国分解数据的分析表明,基本产妇保健服务的获取存在不平等现象。这令人担忧,因为它阻碍了卫生结果的公平进展。要做出有效的反应,就需要确定可能落后的次国家地区。本文旨在探讨产妇保健服务在卫生中心服务范围、村庄和家庭层面的使用的空间变化。还评估了服务使用与家庭财富和妇女教育水平之间的空间相关性。
利用来自在吉马地区三个区参加一项集群随机试验的 3758 户家庭的调查数据,研究了产妇等候之家(MWH)、产前护理(ANC)、分娩护理和产后护理(PNC)的使用在地理上的变化。还使用等值线图在 24 个卫生中心服务范围内探讨了服务使用与教育和财富水平之间的相关性。使用 Moran's I 评估了全球空间自相关。在村庄和家庭层面使用 Getis Ord Gi* 和 Kulldorf 空间扫描统计数据进行聚类分析,以确定聚类位置。
ANC 使用(Moran's I=0.15,p 值=0.025)、分娩护理(Moran's I=0.17,p 值=0.01)和 PNC 使用(Moran's I=0.31,p 值<0.01)存在显著的全球空间自相关,但 MWH 使用没有(Moran's I=-0.005,p 值=0.94),表明具有相似高(热点)和/或低(冷点)服务使用的村庄聚类。在 Gomma 区的卫生中心服务范围内发现了热点,而 Kersa 区则存在冷点。高贫困或低教育服务范围通常服务使用水平较低,但也有例外。在村庄层面,发现了 ANC、分娩护理和 PNC 使用的热点和冷点。家庭层面的分析显示,以前未检测到一个较高的 MWH 使用的主要聚类。需要进一步调查空间异质性。
在吉马地区存在产妇保健服务的次国家差异。在确定服务使用冷点的地区,相对较高的贫困和较低的教育程度。为了确保产妇健康的公平进展,需要将资源重新分配给弱势群体和落后的地点。