Payabyab Eden C, Hemli Jonathan M, Mattia Allan, Kremers Alex, Vatsia Sohrab K, Scheinerman S Jacob, Mihelis Efstathia A, Hartman Alan R, Brinster Derek R
Division of Cardiac Surgery, Virginia Commonwealth University Health Systems, Richmond, VA, USA.
Department of Cardiothoracic Surgery, New York Presbyterian-Weill Cornell Medicine, New York, NY, USA.
J Cardiothorac Surg. 2020 Jul 31;15(1):205. doi: 10.1186/s13019-020-01249-1.
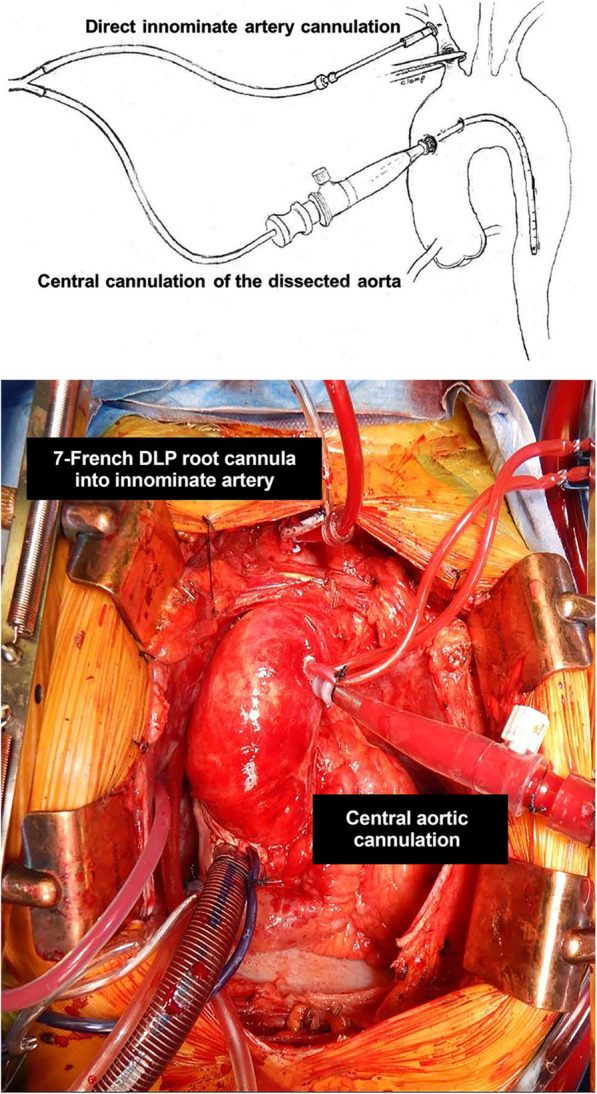
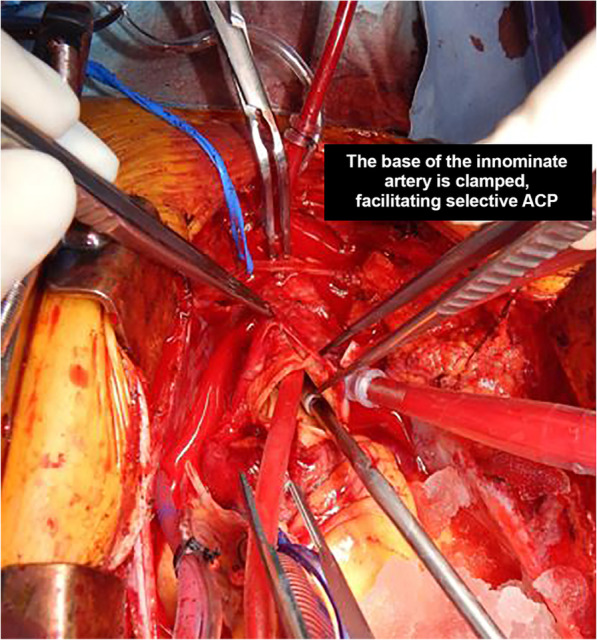
Direct cannulation of the innominate artery for selective antegrade cerebral perfusion has been shown to be safe in elective proximal aortic reconstructions. We sought to evaluate the safety of this technique in acute aortic dissection.
A multi-institutional retrospective review was undertaken of patients who underwent proximal aortic reconstruction for Stanford type A dissection between 2006 and 2016. Those patients who had direct innominate artery cannulation for selective antegrade cerebral perfusion were selected for analysis.
Seventy-five patients underwent innominate artery cannulation for ACP for Stanford Type A Dissections. Isolated replacement of the ascending aorta was performed in 36 patients (48.0%), concomitant aortic root replacement was required in 35 patients (46.7%), of whom 7 had a valve-sparing aortic root replacement, ascending aorta and arch replacement was required in 4 patients (5%). Other procedures included frozen elephant trunk (n = 11 (14.7%)), coronary artery bypass grafting (n = 20 (26.7%)), and peripheral arterial bypass (n = 4 (5.3%)). Mean hypothermic circulatory arrest time was 19 ± 13 min. Thirty-day mortality was 14.7% (n = 11). Perioperative stroke occurred in 7 patients (9.3%).
This study is the first comprehensive review of direct innominate artery cannulation through median sternotomy for selective antegrade cerebral perfusion in aortic dissection. Our experience suggests that this strategy is a safe and effective technique compared to other reported methods of cannulation and cerebral protection for delivering selective antegrade cerebral perfusion in these cases.
在择期近端主动脉重建术中,经无名动脉直接插管进行选择性顺行性脑灌注已被证明是安全的。我们试图评估该技术在急性主动脉夹层中的安全性。
对2006年至2016年间因斯坦福A型夹层而行近端主动脉重建术的患者进行多机构回顾性研究。选择那些经无名动脉直接插管进行选择性顺行性脑灌注的患者进行分析。
75例患者因斯坦福A型夹层经无名动脉插管进行顺行性脑灌注。36例患者(48.0%)单纯行升主动脉置换,35例患者(46.7%)需要同期行主动脉根部置换,其中7例行保留瓣膜的主动脉根部置换,4例患者(5%)需要行升主动脉和主动脉弓置换。其他手术包括冰冻象鼻手术(n = 11(14.7%))、冠状动脉旁路移植术(n = 20(26.7%))和外周动脉旁路移植术(n = 4(5.3%))。平均低温循环阻断时间为19±13分钟。30天死亡率为14.7%(n = 11)。围手术期7例患者(9.3%)发生卒中。
本研究是首次对经正中胸骨切开术经无名动脉直接插管进行主动脉夹层选择性顺行性脑灌注的综合回顾。我们的经验表明,与其他报道的插管和脑保护方法相比,该策略是一种安全有效的技术,可在这些病例中进行选择性顺行性脑灌注。