Centre for Primary Care and Public Health, Queen Mary University of London, London, UK.
NPJ Prim Care Respir Med. 2020 Jul 31;30(1):34. doi: 10.1038/s41533-020-00191-y.
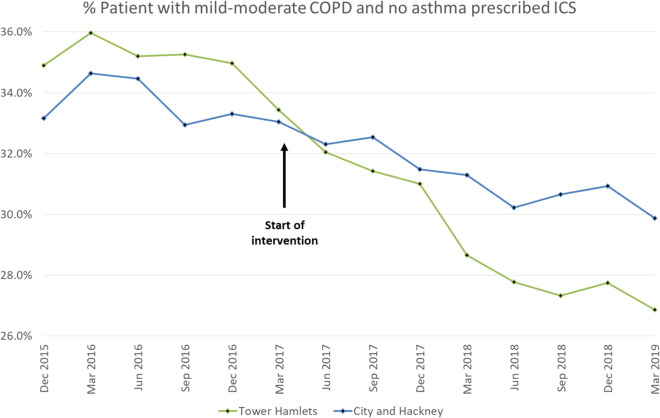
Inhaled corticosteroids (ICS) are often prescribed for worsening breathlessness, exacerbation frequency or lung function in chronic obstructive pulmonary disease (COPD). In mild-moderate disease and infrequent exacerbations, treatment risks may outweigh benefits and ICS may be withdrawn safely under supervision. A systematic ICS deprescribing programme for patients with mild-moderate COPD was introduced in an east London Clinical Commissioning Group (CCG) in April 2017. Primary care patient record analysis found that prescribing fell from 34.9% (n = 701) in the 18 months pre-intervention to 26.9% (n = 538) by the second year of implementation, decreasing 0.84% per quarter post intervention (p = 0.006, linear regression). The relative decrease was greater than the comparison CCG (23.0% vs. 9.9%). Only South Asian ethnicity was associated with increased cessation (odds ratio 1.48, confidence interval (CI) 1.09-2.01), p = 0.013, logistic regression). Patient outcome data were not collected. A primary care-led programme comprising local education, financial incentivisation and consultant support led to a significant decrease in ICS prescribing.
吸入性皮质类固醇(ICS)常用于治疗慢性阻塞性肺疾病(COPD)恶化的呼吸困难、加重频率或肺功能。在轻度至中度疾病和发作不频繁的情况下,治疗风险可能超过获益,并且在监督下可以安全地停用 ICS。2017 年 4 月,在伦敦东部临床委托组(CCG)推出了一项针对轻度至中度 COPD 患者的 ICS 减量计划。初级保健患者病历分析发现,在干预前的 18 个月内,处方从 34.9%(n=701)降至实施第二年的 26.9%(n=538),每季度干预后下降 0.84%(p=0.006,线性回归)。相对减少量大于对照组 CCG(23.0%比 9.9%)。只有南亚种族与停药增加相关(比值比 1.48,置信区间(CI)1.09-2.01,p=0.013,逻辑回归)。未收集患者结局数据。以初级保健为主导的方案包括当地教育、财务激励和顾问支持,导致 ICS 处方显著减少。