Department of Gastro-Intestinal Surgery, Amsterdam University Medical Center, Location VU University, De Boelelaan 1117, ZH 7F020, 1081 HV, Amsterdam, The Netherlands.
Department of Clinical Epidemiology, Amsterdam University Medical Center, Amsterdam, The Netherlands.
Gastric Cancer. 2021 Jan;24(1):258-271. doi: 10.1007/s10120-020-01109-w. Epub 2020 Jul 31.
Surgical resection with adequate lymphadenectomy is regarded the only curative option for gastric cancer. Regarding minimally invasive techniques, mainly Asian studies showed comparable oncological and short-term postoperative outcomes. The incidence of gastric cancer is lower in the Western population and patients often present with more advanced stages of disease. Therefore, the reproducibility of these Asian results in the Western population remains to be investigated.
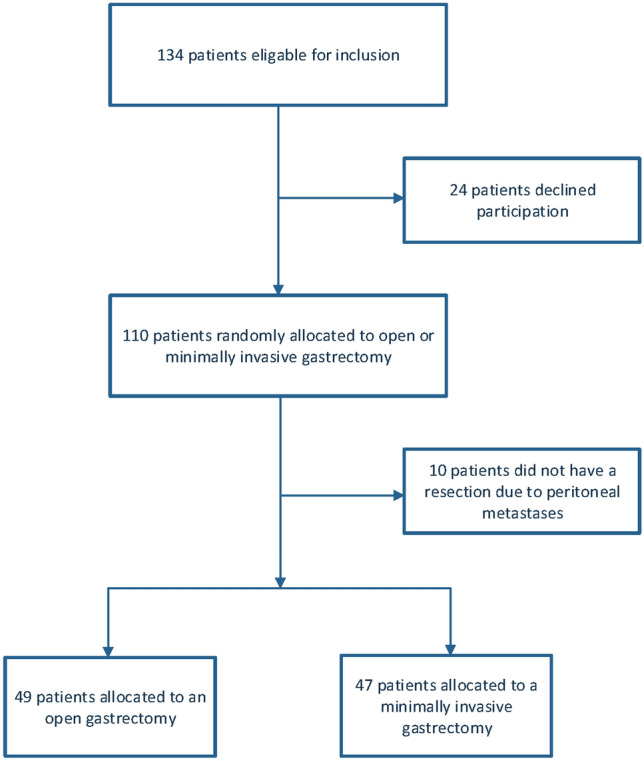
A randomized trial was performed in thirteen hospitals in Europe. Patients with an indication for total gastrectomy who received neoadjuvant chemotherapy were eligible for inclusion and randomized between open total gastrectomy (OTG) or minimally invasive total gastrectomy (MITG). Primary outcome was oncological safety, measured as the number of resected lymph nodes and radicality. Secondary outcomes were postoperative complications, recovery and 1-year survival.
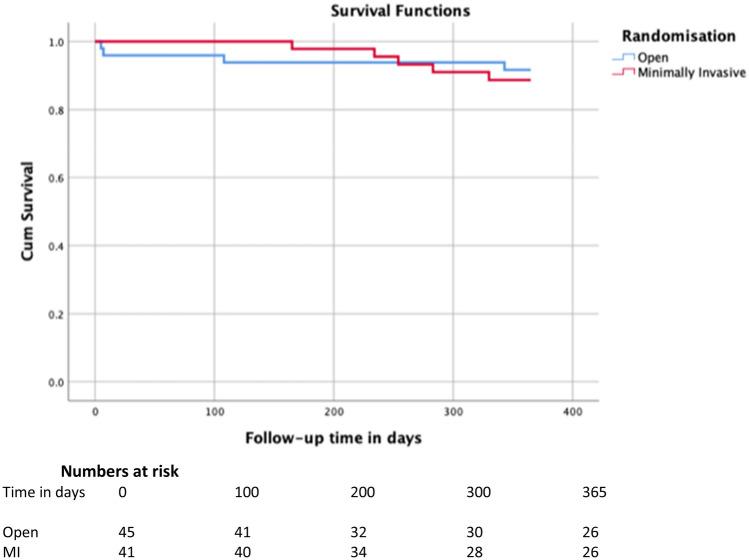
Between January 2015 and June 2018, 96 patients were included in this trial. Forty-nine patients were randomized to OTG and 47 to MITG. The mean number of resected lymph nodes was 43.4 ± 17.3 in OTG and 41.7 ± 16.1 in MITG (p = 0.612). Forty-eight patients in the OTG group had a R0 resection and 44 patients in the MITG group (p = 0.617). One-year survival was 90.4% in OTG and 85.5% in MITG (p = 0.701). No significant differences were found regarding postoperative complications and recovery.
These findings provide evidence that MITG after neoadjuvant therapy is not inferior regarding oncological quality of resection in comparison to OTG in Western patients with resectable gastric cancer. In addition, no differences in postoperative complications and recovery were seen.
手术切除加充分的淋巴结清扫被认为是胃癌的唯一治愈方法。关于微创手术,主要是亚洲的研究表明其具有相当的肿瘤学和短期术后结果。在西方人群中,胃癌的发病率较低,患者往往处于疾病的晚期。因此,这些亚洲研究结果在西方人群中的可重复性仍有待研究。
在欧洲的 13 家医院进行了一项随机试验。接受新辅助化疗的全胃切除术指征患者有资格入选并随机分为开放性全胃切除术(OTG)或微创全胃切除术(MITG)。主要终点是肿瘤学安全性,以切除的淋巴结数量和根治性来衡量。次要终点是术后并发症、恢复情况和 1 年生存率。
2015 年 1 月至 2018 年 6 月期间,本试验纳入了 96 例患者。49 例患者被随机分为 OTG 组,47 例患者被随机分为 MITG 组。OTG 组平均切除淋巴结数为 43.4±17.3 个,MITG 组为 41.7±16.1 个(p=0.612)。OTG 组 48 例患者行 R0 切除术,MITG 组 44 例患者行 R0 切除术(p=0.617)。OTG 组和 MITG 组的 1 年生存率分别为 90.4%和 85.5%(p=0.701)。术后并发症和恢复情况无显著差异。
这些发现为 MITG 在可切除胃癌的西方患者中,在新辅助治疗后在肿瘤学切除质量方面不劣于 OTG 提供了证据。此外,在术后并发症和恢复方面也没有差异。