University of Cincinnati, Cincinnati, Ohio.
SWOG Statistical and Data Management Center, Seattle, Washington.
Ann Surg. 2020 Sep 1;272(3):481-486. doi: 10.1097/SLA.0000000000004155.
The optimal neoadjuvant therapy for resectable pancreatic ductal adenocarcinoma (PDA) and the impact on surgical outcomes remains unclear.
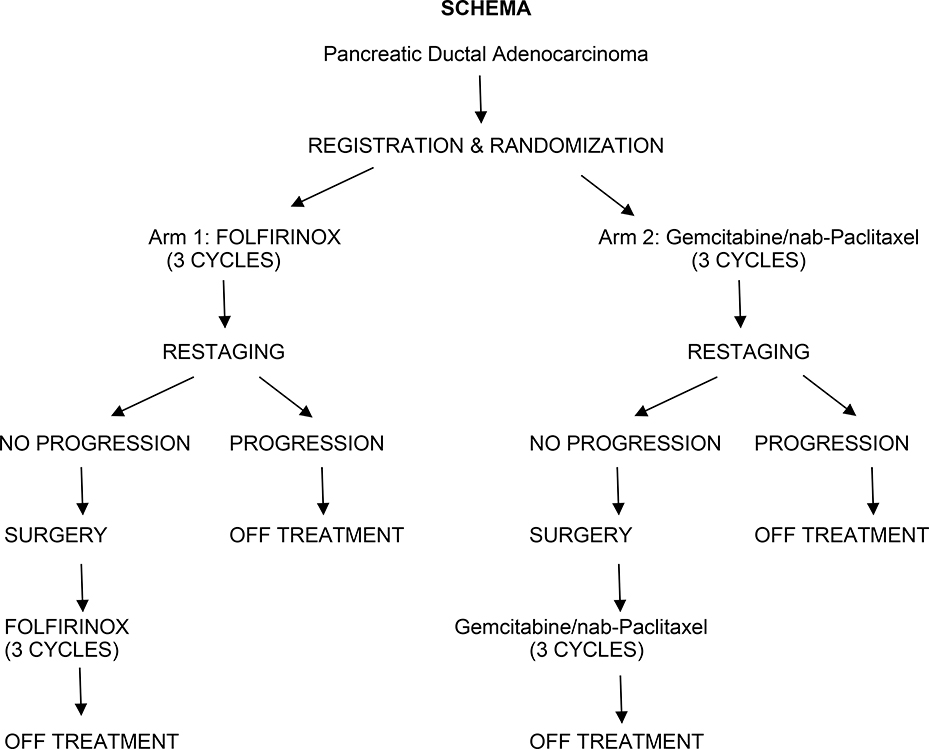
S1505 (NCT02562716) was a randomized phase II study of perioperative chemotherapy with mFOLFIRINOX (Arm 1) or gemcitabine/nab-paclitaxel (Arm 2). Measured parameters included resection rate, margin positivity, pathologic response, and toxicity.
Between 2015 and 2018, 147 patients were randomized. Of these, 44 (30%) were deemed ineligible (43 by central review). Of the 103 eligible patients, 77 (76%) completed preoperative therapy and underwent surgery; reasons patients did not undergo surgery included toxicity related to preoperative therapy (n = 9), progression (n = 9), or other (n = 7). Of the 77, 73 (95%) underwent successful resection; 21 (29%) required vascular reconstruction, 62 (85%) had negative (R0) margins, and 24 (33%) had a complete or major pathologic response to therapy. The grade 3-5 postoperative complication rate was 16%. Of the 73 patients completing surgery, 57 (78%) started and 46 (63%) completed postoperative therapy. This study represents the first prospective trial evaluating modern systemic therapy delivered in a neoadjuvant/perioperative format for resectable PDA.
We have demonstrated: (1) Based on the high percentage of enrolled, but ineligible patients, it is clear that adherence to strict definitions of resectable PDA is challenging; (2) Patients can tolerate modern systemic therapy and undergo successful surgical resection without prohibitive perioperative complications; (3) Completion of adjuvant therapy in the perioperative format is difficult; (4) Major pathologic response rate of 33% is encouraging.
可切除胰腺导管腺癌(PDA)的最佳新辅助治疗方法及其对手术结果的影响仍不清楚。
S1505(NCT02562716)是一项关于围手术期化疗的随机 II 期研究,使用 mFOLFIRINOX(A 组)或吉西他滨/ nab-紫杉醇(B 组)。测量参数包括切除率、边缘阳性率、病理反应和毒性。
2015 年至 2018 年间,共随机分配了 147 例患者。其中,44 例(30%)被认为不符合条件(43 例经中心审查)。在 103 例合格患者中,77 例(76%)完成了术前治疗并接受了手术;未行手术的患者原因包括术前治疗相关毒性(n=9)、进展(n=9)或其他(n=7)。在 77 例患者中,73 例(95%)成功进行了切除;21 例(29%)需要血管重建,62 例(85%)边缘阴性(R0),24 例(33%)对治疗有完全或主要的病理反应。术后 3-5 级并发症发生率为 16%。在完成手术的 73 例患者中,57 例(78%)开始并完成了 46 例(63%)术后治疗。本研究代表了首例前瞻性试验,评估了可切除 PDA 的新辅助/围手术期应用现代系统治疗。
我们已经证明:(1)根据入组但不符合条件的患者的高百分比,显然严格定义可切除 PDA 具有挑战性;(2)患者可以耐受现代系统治疗,并在没有明显围手术期并发症的情况下成功进行手术切除;(3)在围手术期模式下完成辅助治疗很困难;(4)33%的主要病理反应率令人鼓舞。