Lindenmeyer Christina C, Flocco Gianina, Sanghi Vedha, Lopez Rocio, Kim Ahyoung J, Niyazi Fadi, Mehta Neal A, Kapoor Aanchal, Carey William D, Mireles-Cabodevila Eduardo, Romero-Marrero Carlos
Department of Gastroenterology, Hepatology and Nutrition, Cleveland Clinic, Cleveland, OH 44195, United States.
Department of Internal Medicine, Cleveland Clinic, Cleveland, OH 44195, United States.
World J Hepatol. 2020 Jun 27;12(6):298-311. doi: 10.4254/wjh.v12.i6.298.
Critically ill patients with cirrhosis, particularly those with acute decompensation, have higher mortality rates in the intensive care unit (ICU) than patients without chronic liver disease. Prognostication of short-term mortality is important in order to identify patients at highest risk of death. None of the currently available prognostic models have been widely accepted for use in cirrhotic patients in the ICU, perhaps due to complexity of calculation, or lack of universal variables readily available for these patients. We believe a survival model meeting these requirements can be developed, to guide therapeutic decision-making and contribute to cost-effective healthcare resource utilization.
To identify markers that best identify likelihood of survival and to determine the performance of existing survival models.
Consecutive cirrhotic patients admitted to a United States quaternary care center ICU between 2008-2014 were included and comprised the training cohort. Demographic data and clinical laboratory test collected on admission to ICU were analyzed. Area under the curve receiver operator characteristics (AUROC) analysis was performed to assess the value of various scores in predicting in-hospital mortality. A new predictive model, the LIV-4 score, was developed using logistic regression analysis and validated in a cohort of patients admitted to the same institution between 2015-2017.
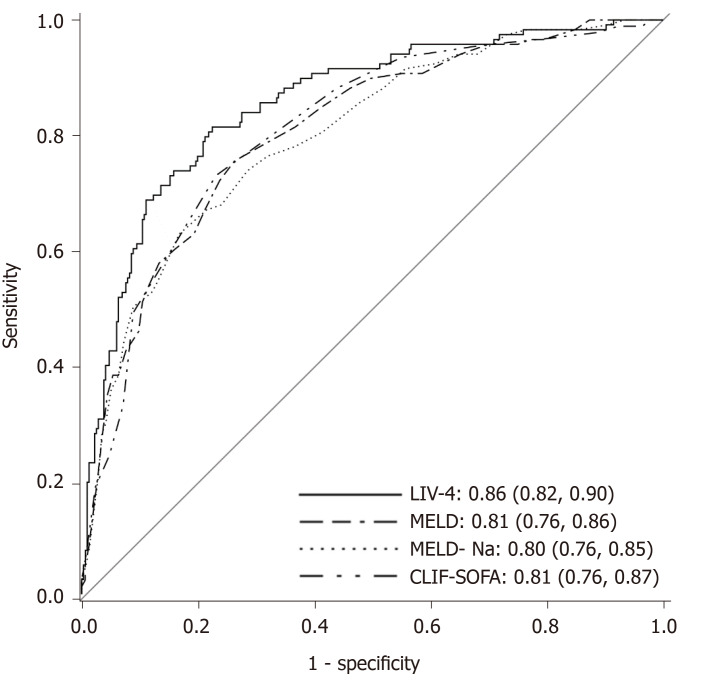
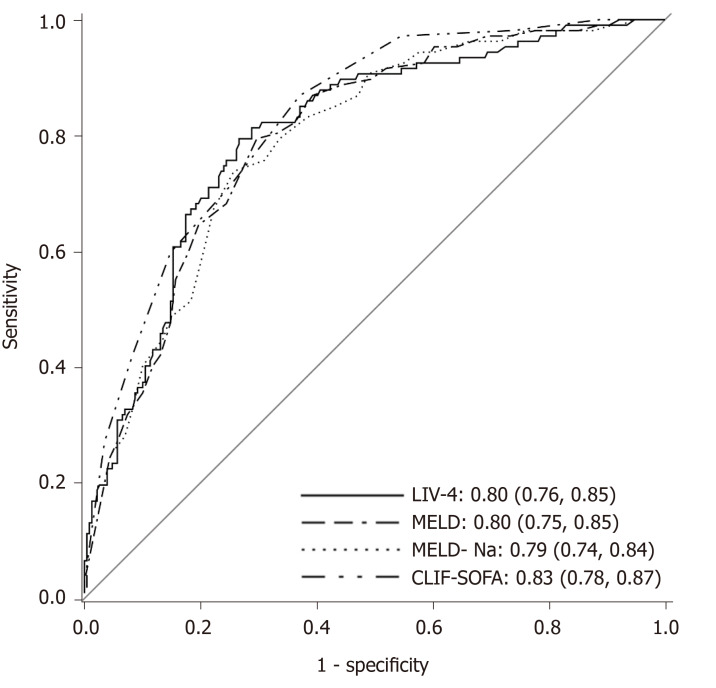
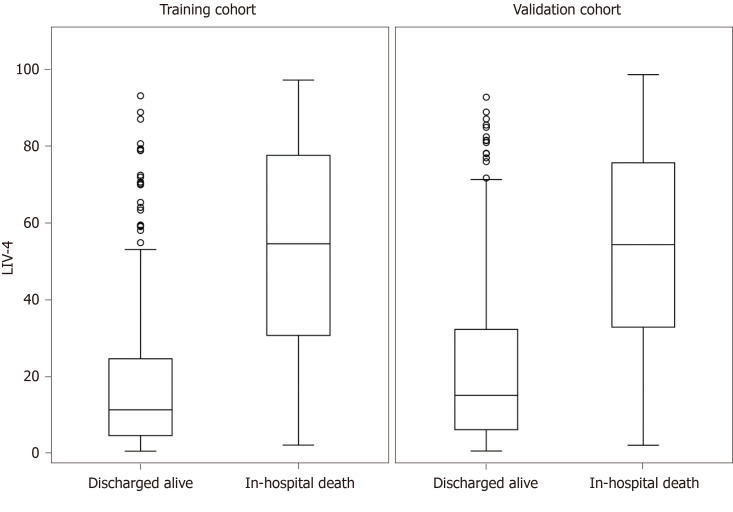
Of 436 patients, 119 (27.3%) died in the hospital. In multivariate analysis, a combination of the natural logarithm of the bilirubin, prothrombin time, white blood cell count, and mean arterial pressure was found to most accurately predict in-hospital mortality. Derived from the regression coefficients of the independent variables, a novel model to predict inpatient mortality was developed (the LIV-4 score) and performed with an AUROC of 0.86, compared to the Model for End-Stage Liver Disease, Chronic Liver Failure-Sequential Organ Failure Assessment, and Royal Free Hospital Score, which performed with AUROCs of 0.81, 0.80, and 0.77, respectively. Patients in the internal validation cohort were substantially sicker, as evidenced by higher Model for End-Stage Liver Disease, Model for End-Stage Liver Disease-Sodium, Acute Physiology and Chronic Health Evaluation III, SOFA and LIV-4 scores. Despite these differences, the LIV-4 score remained significantly higher in subjects who expired during the hospital stay and exhibited good prognostic values in the validation cohort with an AUROC of 0.80.
LIV-4, a validated model for predicting mortality in cirrhotic patients on admission to the ICU, performs better than alternative liver and ICU-specific survival scores.
肝硬化重症患者,尤其是急性失代偿患者,在重症监护病房(ICU)的死亡率高于无慢性肝病的患者。预测短期死亡率对于识别死亡风险最高的患者很重要。目前可用的预后模型均未被广泛接受用于ICU中的肝硬化患者,这可能是由于计算复杂,或者缺乏适用于这些患者的通用变量。我们相信可以开发出满足这些要求的生存模型,以指导治疗决策并促进具有成本效益的医疗资源利用。
识别最能确定生存可能性的标志物,并确定现有生存模型的性能。
纳入2008年至2014年间入住美国一家四级医疗中心ICU的连续性肝硬化患者,组成训练队列。分析入住ICU时收集的人口统计学数据和临床实验室检查结果。进行曲线下面积接受者操作特征(AUROC)分析,以评估各种评分在预测院内死亡率方面的价值。使用逻辑回归分析开发了一种新的预测模型,即LIV-4评分,并在2015年至2017年间入住同一机构的患者队列中进行了验证。
436例患者中,119例(27.3%)死于医院。在多变量分析中,发现胆红素的自然对数、凝血酶原时间、白细胞计数和平均动脉压的组合最能准确预测院内死亡率。根据自变量的回归系数,开发了一种预测住院死亡率的新模型(LIV-4评分),其AUROC为0.86,而终末期肝病模型、慢性肝功能衰竭-序贯器官衰竭评估模型和皇家自由医院评分的AUROC分别为0.81、0.80和0.77。内部验证队列中的患者病情严重得多,终末期肝病模型、终末期肝病-钠模型、急性生理与慢性健康状况评估III、序贯器官衰竭评估和LIV-4评分更高证明了这一点。尽管存在这些差异,LIV-4评分在住院期间死亡的患者中仍然显著更高,并且在验证队列中表现出良好的预后价值,AUROC为0.80。
LIV-4是一种经过验证的模型,用于预测肝硬化患者入住ICU时的死亡率,其性能优于其他肝脏和ICU特异性生存评分。