Department of Psychiatry, Psychotherapy and Psychosomatics, Psychiatric Hospital, University of Zurich, Zurich, Switzerland.
McConnell Brain Imaging Centre, Montréal Neurological Institute, McGill University, Montreal, Canada.
Schizophr Bull. 2020 Dec 1;46(6):1426-1438. doi: 10.1093/schbul/sbaa097.
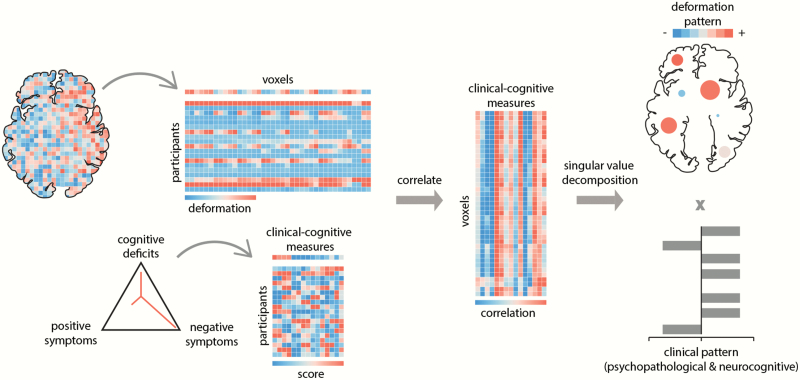
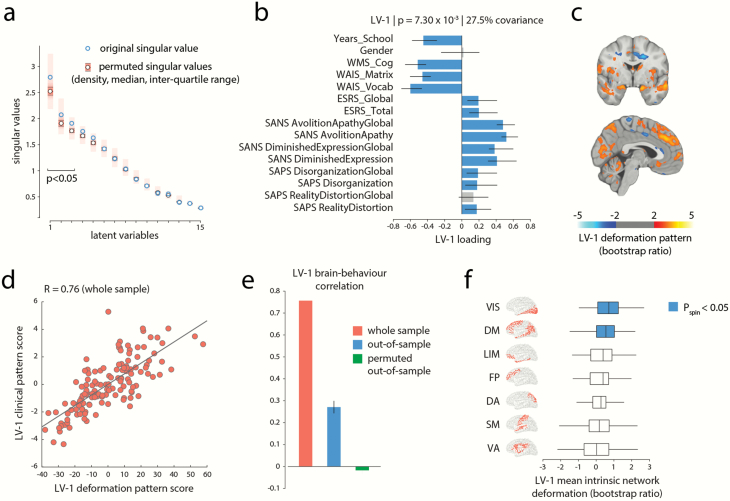
Widespread structural brain abnormalities have been consistently reported in schizophrenia, but their relation to the heterogeneous clinical manifestations remains unknown. In particular, it is unclear whether anatomical abnormalities in discrete regions give rise to discrete symptoms or whether distributed abnormalities give rise to the broad clinical profile associated with schizophrenia. Here, we apply a multivariate data-driven approach to investigate covariance patterns between multiple-symptom domains and distributed brain abnormalities in schizophrenia. Structural magnetic resonance imaging and clinical data were derived from one discovery sample (133 patients and 113 controls) and one independent validation sample (108 patients and 69 controls). Disease-related voxel-wise brain abnormalities were estimated using deformation-based morphometry. Partial least-squares analysis was used to comprehensively map clinical, neuropsychological, and demographic data onto distributed deformation in a single multivariate model. The analysis identified 3 latent clinical-anatomical dimensions that collectively accounted for 55% of the covariance between clinical data and brain deformation. The first latent clinical-anatomical dimension was replicated in an independent sample, encompassing cognitive impairments, negative symptom severity, and brain abnormalities within the default mode and visual networks. This cognitive-negative dimension was associated with low socioeconomic status and was represented across multiple races. Altogether, we identified a continuous cognitive-negative dimension of schizophrenia, centered on 2 intrinsic networks. By simultaneously taking into account both clinical manifestations and neuroanatomical abnormalities, the present results open new avenues for multi-omic stratification and biotyping of individuals with schizophrenia.
广泛性的结构性脑异常在精神分裂症中一直被一致报道,但它们与异质的临床表现之间的关系尚不清楚。特别是,尚不清楚离散区域的解剖学异常是否会导致离散的症状,或者分布性异常是否会导致与精神分裂症相关的广泛临床特征。在这里,我们应用一种多变量数据驱动的方法来研究精神分裂症中多个症状领域与分布性脑异常之间的协变模式。结构磁共振成像和临床数据来自一个发现样本(133 名患者和 113 名对照)和一个独立的验证样本(108 名患者和 69 名对照)。使用基于变形的形态测量法来估计与疾病相关的体素级别的脑异常。偏最小二乘分析用于在单个多变量模型中将临床、神经心理学和人口统计学数据综合映射到分布性变形上。该分析确定了 3 个潜在的临床解剖学维度,它们共同解释了临床数据和大脑变形之间 55%的协方差。第一个潜在的临床解剖学维度在独立样本中得到了复制,包含认知障碍、阴性症状严重程度以及默认模式和视觉网络内的脑异常。这个认知-阴性维度与低社会经济地位有关,并且存在于多种种族中。总之,我们确定了一个以 2 个内在网络为中心的精神分裂症连续的认知-阴性维度。通过同时考虑临床表现和神经解剖异常,本研究结果为精神分裂症患者的多组学分层和生物分型开辟了新的途径。