University of Lille, Inserm, Lille, France.
CHU Lille, Neuro-oncology, General and Stereotaxic Neurosurgery service, Lille, France.
ESMO Open. 2020 Aug;5(4). doi: 10.1136/esmoopen-2020-000763.
The optimal sequence of stereotactic radiotherapy (SRT) and immune checkpoint inhibition (ICI) and assessment of response in patients with brain metastases from melanoma remain challenging.
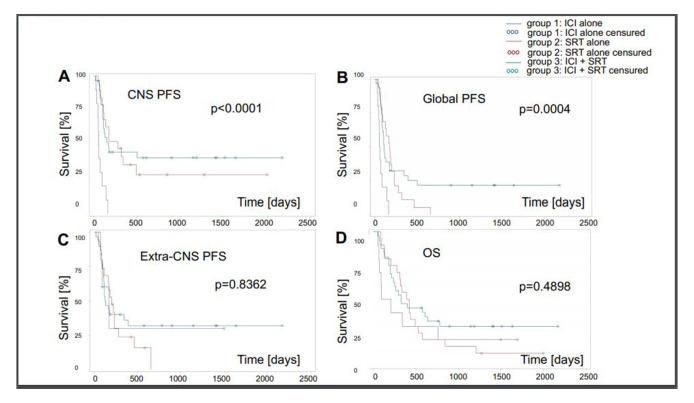
We reviewed clinical and neuroimaging data of 62 patients with melanoma, including 26 patients with BRAF-mutant tumours, with newly diagnosed brain metastases treated with ICI alone (n=10, group 1), SRT alone or in combination with other systemic therapies (n=20, group 2) or ICI plus SRT (n=32, group 3). Response was assessed retrospectively using response evaluation criteria in solid tumours (RECIST) V.1.1, response assessment in neuro-oncology (RANO) and immunotherapy RANO (iRANO) criteria. MRI follow-up from 43 patients was available for central review.
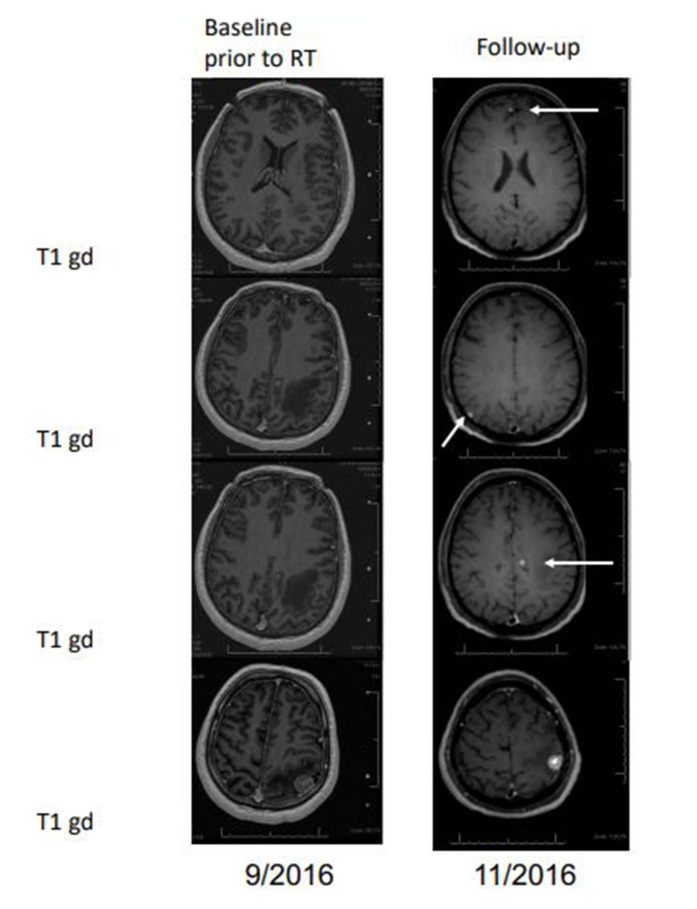
Patients treated with ICI alone showed no objective responses and had worse outcome than patients treated with SRT without or with ICI. RECIST, RANO and iRANO criteria were concordant for complete response (CR) and partial response (PR). RANO called progression earlier than RECIST for clinical deterioration without MRI progression in some patients. Progression was called later when using iRANO criteria because of the need for a confirmatory scan. Pseudoprogression was documented in seven patients: three patients in group 2 and four patients in group 3. Radionecrosis was documented in seven patients: two patients in group 2 and five patients in group 3. Regression of non-irradiated lesions was seen neither in two patients treated with SRT alone nor in five patients treated with SRT plus ICI, providing no evidence for rare abscopal effects.
Pseudoprogression is uncommon with ICI alone, suggesting that growing lesions in such patients should trigger an intervention. Pseudoprogression rates were similar after SRT alone or SRT in combination with ICI. Abscopal effects are rare or do not exist. Response assessment criteria should be considered carefully when designing clinical studies for patients with brain metastases who receive SRT.
立体定向放疗(SRT)和免疫检查点抑制(ICI)的最佳顺序以及评估黑素瘤脑转移患者的反应仍然具有挑战性。
我们回顾了 62 例新发脑转移黑素瘤患者的临床和神经影像学资料,包括 26 例 BRAF 突变肿瘤患者,这些患者单独接受 ICI 治疗(n=10,组 1)、单独接受 SRT 或联合其他全身治疗(n=20,组 2)或 ICI 联合 SRT(n=32,组 3)。使用实体瘤反应评估标准(RECIST)V.1.1、神经肿瘤反应评估(RANO)和免疫治疗 RANO(iRANO)标准对反应进行回顾性评估。对 43 例患者的 MRI 随访结果进行了中心审查。
单独接受 ICI 治疗的患者没有客观反应,且预后比未接受或接受 ICI 联合 SRT 治疗的患者更差。RECIST、RANO 和 iRANO 标准对完全缓解(CR)和部分缓解(PR)的评估一致。在一些患者中,虽然没有 MRI 进展,但出现临床恶化,RANO 比 RECIST 更早地判断为进展。使用 iRANO 标准时,由于需要进行确认性扫描,进展的判断会较晚。7 例患者记录为假性进展:2 例患者在组 2,4 例患者在组 3。7 例患者记录为放射性坏死:2 例患者在组 2,5 例患者在组 3。单独接受 SRT 治疗的 2 例患者和 SRT 联合 ICI 治疗的 5 例患者均未见非照射病灶的消退,这提示罕见的远隔效应并不存在。
单独使用 ICI 时假性进展不常见,这表明此类患者生长的病变应触发干预措施。单独接受 SRT 或 SRT 联合 ICI 治疗后,假性进展的发生率相似。远隔效应罕见或不存在。在设计接受 SRT 的脑转移患者的临床研究时,应仔细考虑评估标准。