Taylor Guy S, Smith Kieran, Capper Tess E, Scragg Jadine H, Bashir Ayat, Flatt Anneliese, Stevenson Emma J, McDonald Timothy J, Oram Richard A, Shaw James A, West Daniel J
Population Health Sciences Institute, Newcastle University, Newcastle upon Tyne, U.K.
Centre for Public Health, Queen's University Belfast, Belfast, U.K.
Diabetes Care. 2020 Oct;43(10):2362-2370. doi: 10.2337/dc20-0300. Epub 2020 Aug 3.
To investigate the impact of residual β-cell function on continuous glucose monitoring (CGM) outcomes following acute exercise in people with type 1 diabetes (T1D).
Thirty participants with T1D for ≥3 years were recruited. First, participants wore a blinded CGM unit for 7 days of free-living data capture. Second, a 3-h mixed-meal test assessed stimulated C-peptide and glucagon. Peak C-peptide was used to allocate participants into undetectable (Cpep <3 pmol/L), low (Cpep 3-200 pmol/L), or high (Cpep >200 pmol/L) C-peptide groups. Finally, participants completed 45 min of incline treadmill walking at 60% VO followed by a further 48-h CGM capture.
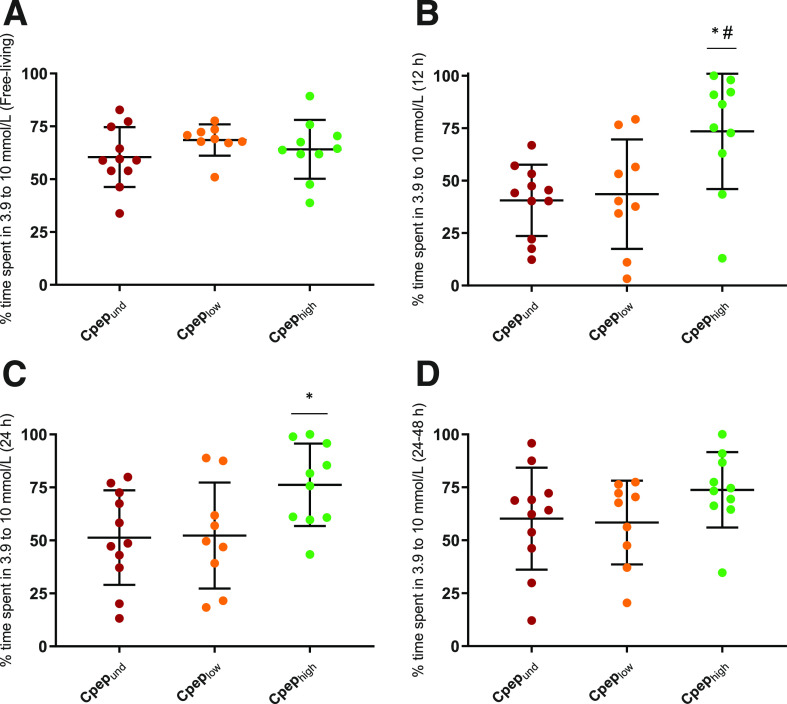
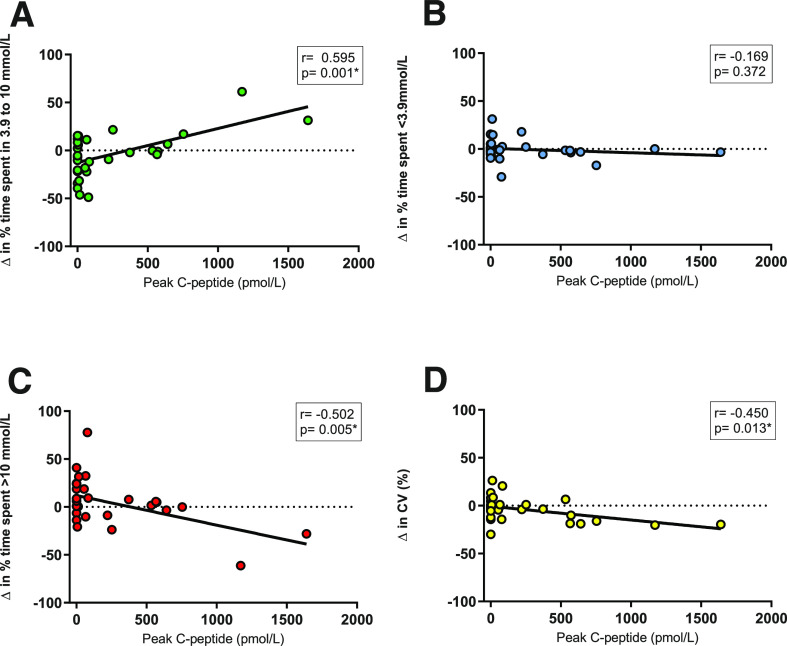
CGM parameters were comparable across groups during the free-living observation week. In the 12- and 24-h postexercise periods (12 h and 24 h), the Cpep group had a significantly greater amount of time spent with glucose 3.9-10 mmol/L (12 h, 73.5 ± 27.6%; 24 h, 76.3 ± 19.2%) compared with Cpep (12 h, 43.6 ± 26.1%, = 0.027; 24 h, 52.3 ± 25.0%, = 0.067) or Cpep (12 h, 40.6 ± 17.0%, = 0.010; 24 h, 51.3 ± 22.3%, = 0.041). Time spent in hyperglycemia (12 h and 24 h glucose >10 and >13.9 mmol/L, < 0.05) and glycemic variability (12 h and 24 h SD, < 0.01) were significantly lower in the Cpep group compared with Cpep and Cpep. Change in CGM outcomes from pre-exercise to 24-h postexercise was divergent: Cpep and Cpep experienced worsening (glucose 3.9-10 mmol/L: -9.1% and -16.2%, respectively), with Cpep experiencing improvement (+12.1%) ( = 0.017).
Residual β-cell function may partially explain the interindividual variation in the acute glycemic benefits of exercise in individuals with T1D. Quantifying C-peptide could aid in providing personalized and targeted support for exercising patients.
探讨1型糖尿病(T1D)患者急性运动后残余β细胞功能对持续葡萄糖监测(CGM)结果的影响。
招募了30名患T1D≥3年的参与者。首先,参与者佩戴盲法CGM设备7天,以收集自由生活状态下的数据。其次,进行3小时的混合餐试验,评估刺激后的C肽和胰高血糖素。根据峰值C肽将参与者分为不可检测(Cpep<3 pmol/L)、低(Cpep 3 - 200 pmol/L)或高(Cpep>200 pmol/L)C肽组。最后,参与者在60%VO₂强度下在倾斜跑步机上行走45分钟,随后再进行48小时的CGM数据收集。
在自由生活观察周期间,各小组的CGM参数具有可比性。在运动后12小时和24小时,与Cpep组(12小时,43.6±26.1%,P = 0.027;24小时,52.3±25.0%,P = 0.067)或Cpep组(12小时,40.6±17.0%,P = 0.010;24小时,51.3±22.3%,P = 0.041)相比,Cpep组血糖在3.9 - 10 mmol/L的时间显著更长(12小时,73.5±27.6%;24小时,76.3±19.2%)。与Cpep组和Cpep组相比,Cpep组高血糖时间(12小时和24小时血糖>10和>13.9 mmol/L,P<0.05)和血糖变异性(12小时和24小时标准差,P<0.01)显著更低。从运动前到运动后24小时,CGM结果的变化存在差异:Cpep组和Cpep组情况恶化(血糖3.9 - 10 mmol/L:分别下降9.1%和16.2%),而Cpep组有所改善(上升12.1%)(P = 0.017)。
残余β细胞功能可能部分解释了T1D患者运动后急性血糖获益的个体间差异。量化C肽有助于为运动患者提供个性化和有针对性的支持。