Department of Neurology, Center of Cerebrovascular Diseases, West China Hospital, Sichuan University, No. 37 GuoXue Xiang, Chengdu, 610041, Sichuan Province, People's Republic of China.
Department of Neurology, People's Hospital of Deyang City, No. 173, North Taishan Road, Deyang, 618000, Sichuan Province, People's Republic of China.
Sci Rep. 2020 Aug 5;10(1):13170. doi: 10.1038/s41598-020-70172-1.
Impaired consciousness (IC) at stroke onset in large hemispheric infarctions (LHI) patients is common in clinical practice. However, little is known about the incidence and risk factors of IC at stroke onset in LHI. Besides, stroke-related complications and clinical outcomes in relation to the development of IC has not been systematically examined. Data of 256 consecutive patients with LHI were collected. IC at stroke onset was retrospectively collected from the initial emergency department and/or admission records. Of the 256 LHI patients enrolled, 93 (36.3%) had IC at stroke onset. LHI patients with IC at stroke onset were older (median age 66 vs. 61, p = 0.041), had shorter prehospital delay (24 vs. 26 h, p < 0.001and higher baseline National Institutes of Health Stroke Scale (NIHSS) score (19 vs. 12, p < 0.001). Independent risk factors of IC at stroke onset were high NIHSS score (odds ratio, OR 1.17, 95% confidence interval [CI] 1.12 to 1.23) and atrial fibrillation (OR 1.93, 95% CI 1.07 to 3.47). Dyslipidemia appeared to protect against IC at stroke onset (adjusted OR 0.416, 95% CI 0.175 to 0.988). IC at stroke onset was associated with higher frequency of stroke-related complications (90.32% vs. 67.48%, p < 0.001), especially brain edema (45.16% vs. 23.31%, p < 0.001) and pneumonia (63.44% vs. 47.82%, p = 0.019). The IC group had higher rates of in-hospital death (23.66% vs. 11.66%, p = 0.012), 3-month mortality (49.46% vs. 24.87%, p = 0.002), and 3-month unfavorable outcome (64.51% vs. 49.07%, p = 0.017). However, after adjusting for age, baseline NIHSS score and other confounders, IC at stroke onset was not an independent predictor of in-hospital death (adjusted OR 0.56, 95% CI 0.22 to 1.47), 3-month mortality (adjusted OR 0.54, 95% CI 0.25 to 1.14) and 3-month unfavorable outcome (adjusted OR 0.64, 95% CI 0.31 to 1.33) in LHI patients (all p > 0.05). Our results suggested that IC occur in 1 out of every 3 LHI patients at stroke onset and was associated with initial stroke severity and atrial fibrillation. LHI patients with IC at stroke onset more frequently had stroke-related complications, 3-month mortality and unfavorable outcome, whereas IC was not an independent predictor of poor outcomes.
在大半球梗死(LHI)患者的卒中发病时出现意识障碍(IC)在临床实践中很常见。然而,对于 LHI 患者卒中发病时 IC 的发生率和危险因素知之甚少。此外,与 IC 发展相关的卒中相关并发症和临床结局尚未系统检查。
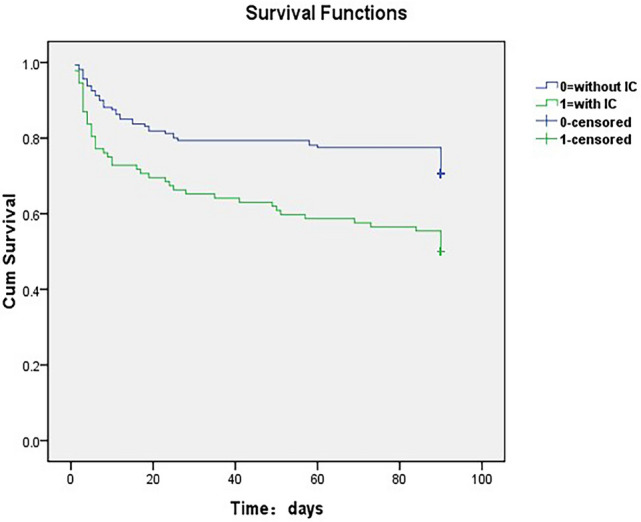
共收集了 256 例连续的 LHI 患者的数据。IC 于卒中发病时从初始急诊室和/或入院记录中回顾性采集。256 例 LHI 患者中,93 例(36.3%)于卒中发病时存在 IC。与卒中发病时无 IC 的患者相比,有 IC 的 LHI 患者年龄更大(中位数年龄 66 岁 vs. 61 岁,p=0.041),发病前的延误时间更短(24 小时 vs. 26 小时,p<0.001),基线国立卫生研究院卒中量表(NIHSS)评分更高(19 分 vs. 12 分,p<0.001)。卒中发病时 IC 的独立危险因素是 NIHSS 评分较高(比值比,OR 1.17,95%置信区间 [CI] 1.12 至 1.23)和心房颤动(OR 1.93,95%CI 1.07 至 3.47)。血脂异常似乎可以预防卒中发病时的 IC(校正 OR 0.416,95%CI 0.175 至 0.988)。卒中发病时存在 IC 与更高频率的卒中相关并发症相关(90.32% vs. 67.48%,p<0.001),尤其是脑水肿(45.16% vs. 23.31%,p<0.001)和肺炎(63.44% vs. 47.82%,p=0.019)。IC 组的院内死亡率(23.66% vs. 11.66%,p=0.012)、3 个月死亡率(49.46% vs. 24.87%,p=0.002)和 3 个月不良结局(64.51% vs. 49.07%,p=0.017)均较高。然而,在校正年龄、基线 NIHSS 评分和其他混杂因素后,卒中发病时的 IC 并不是 LHI 患者院内死亡(校正 OR 0.56,95%CI 0.22 至 1.47)、3 个月死亡率(校正 OR 0.54,95%CI 0.25 至 1.14)和 3 个月不良结局(校正 OR 0.64,95%CI 0.31 至 1.33)的独立预测因素(均 p>0.05)。
我们的结果表明,LHI 患者中每 3 例就有 1 例于卒中发病时出现 IC,与初始卒中严重程度和心房颤动相关。卒中发病时存在 IC 的 LHI 患者更常出现卒中相关并发症、3 个月死亡率和不良结局,而 IC 并不是不良结局的独立预测因素。