Department of Pediatrics, Vanderbilt University Medical Center, 2146 Belcourt Avenue, Nashville TN 37212, USA; Department of Health Policy, Vanderbilt University Medical Center, 1500 21st Ave S, Suite 2600, Nashville TN 37212, USA.
Department of Pediatrics, Vanderbilt University Medical Center, 2146 Belcourt Avenue, Nashville TN 37212, USA.
Environ Int. 2020 Oct;143:105970. doi: 10.1016/j.envint.2020.105970. Epub 2020 Jul 30.
Previous studies of prenatal phthalate exposure and childhood asthma are inconsistent. These studies typically model phthalates as individual, rather than co-occurring, exposures. We investigated whether prenatal phthalates are associated with childhood wheeze and asthma using a mixtures approach.
We studied dyads from two prenatal cohorts in the ECHO-PATHWAYS consortium: CANDLE, recruited 2006-2011 and TIDES, recruited 2011-2013. Parents reported child respiratory outcomes at age 4-6 years: ever asthma, current wheeze (symptoms in past 12 months) and current asthma (two affirmative responses from ever asthma, recent asthma-specific medication use, and/or current wheeze). We quantified 11 phthalate metabolites in third trimester urine and estimated associations with child respiratory outcomes using weighted quantile sum (WQS) logistic regression, using separate models to estimate protective and adverse associations, adjusting for covariates. We examined effect modification by child sex and maternal asthma.
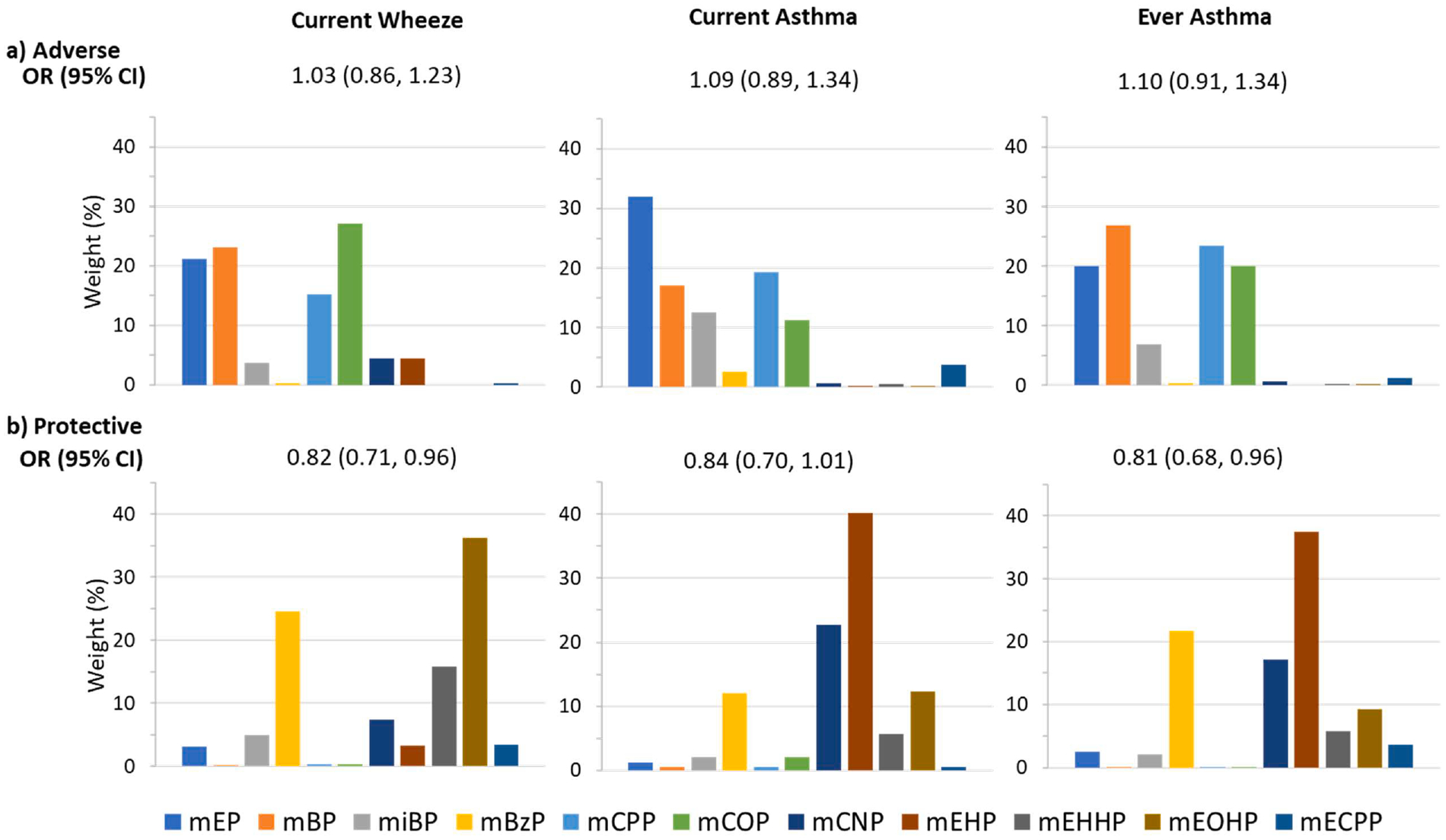
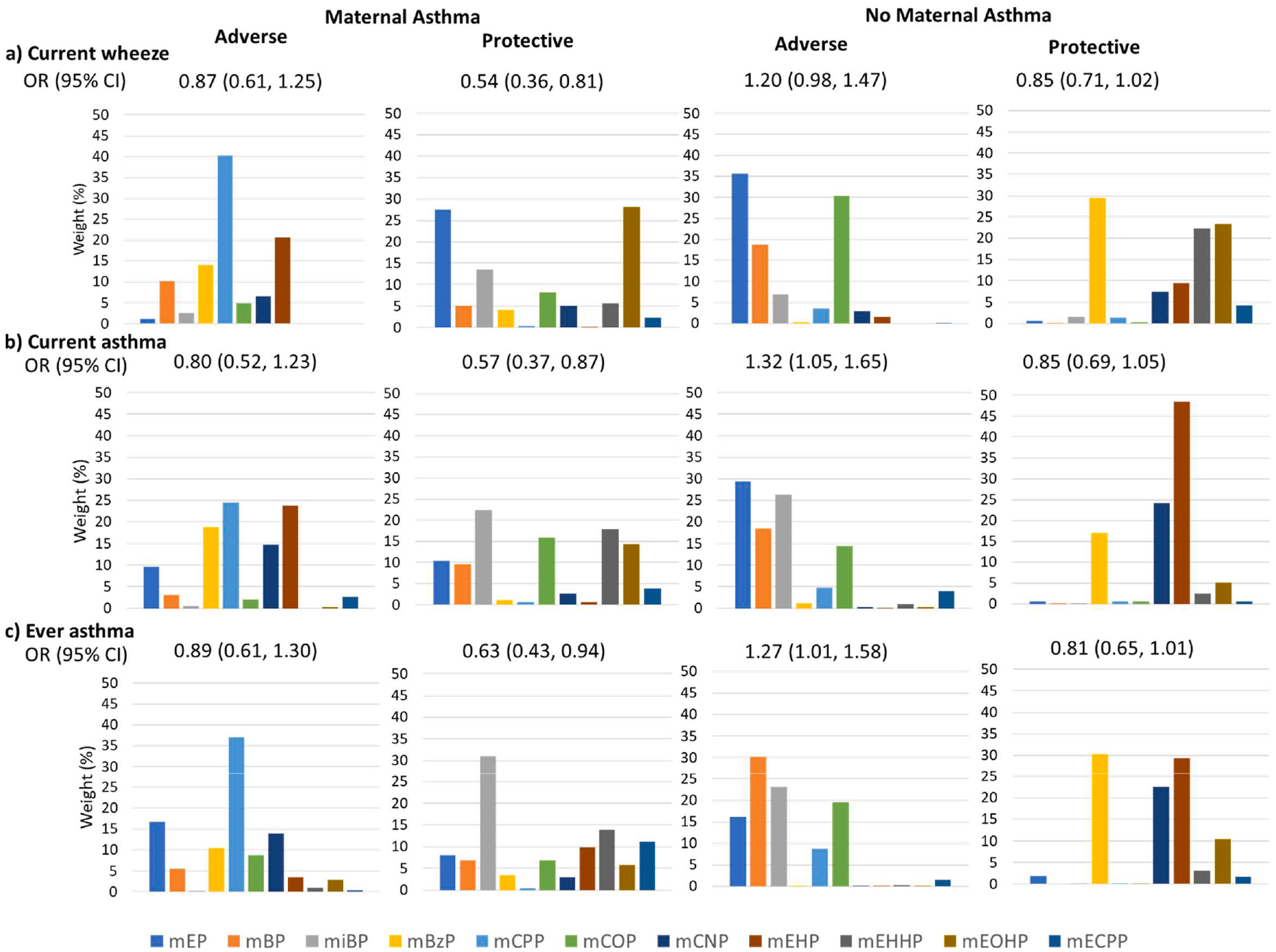
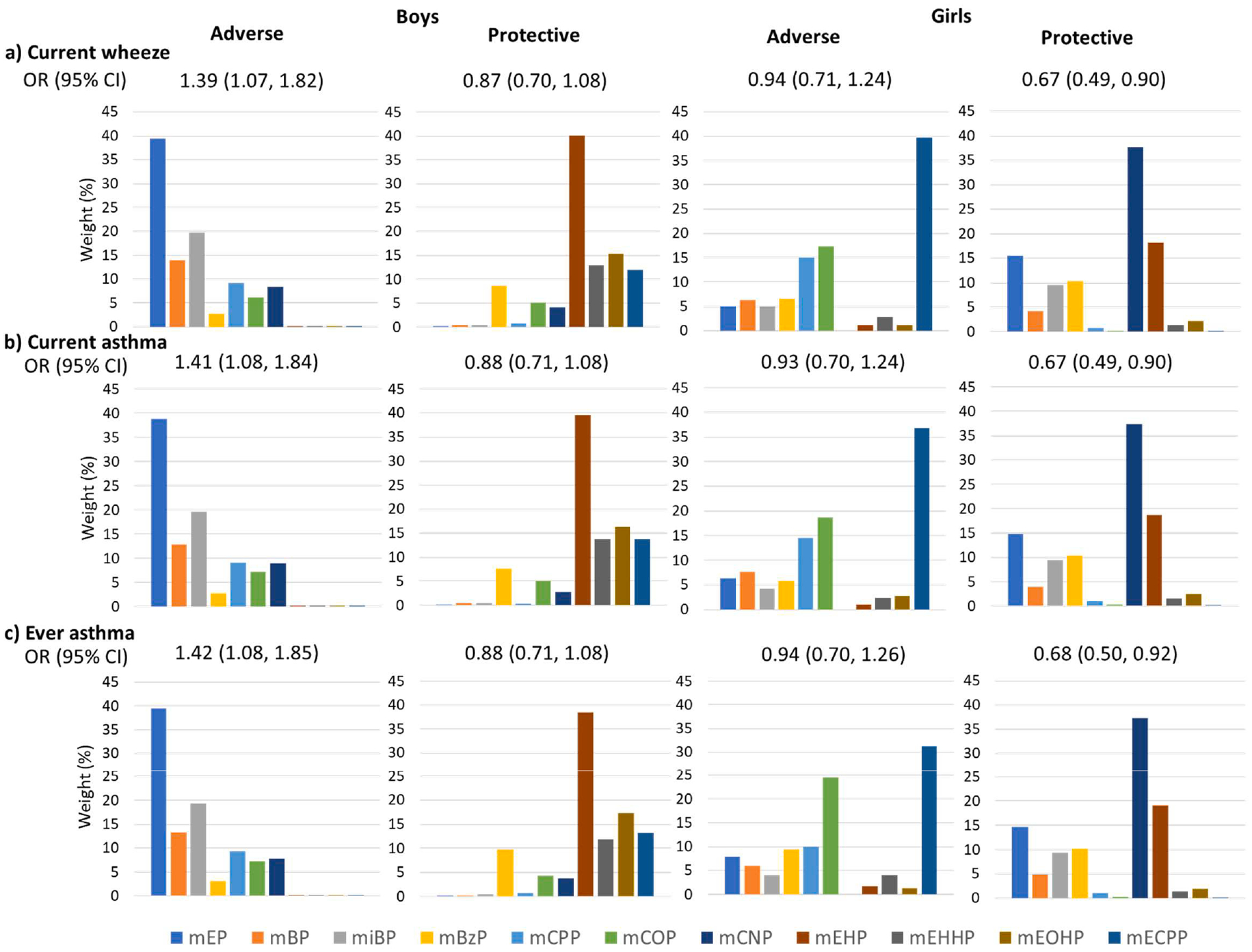
Of 1481 women, most identified as White (46.6%) or Black (44.6%); 17% reported an asthma history. Prevalence of ever asthma, current wheeze and current asthma in children was 12.3%, 15.8% and 12.3%, respectively. Overall, there was no adverse association with respiratory outcomes. In sex-stratified analyses, boys' phthalate index was adversely associated with all outcomes (e.g., boys' ever asthma: adjusted odds ratio per one quintile increase in WQS phthalate index (AOR): 1.42; 95% confidence interval (CI): 1.08, 1.85, with mono-ethyl phthalate (MEP) weighted highest). Adverse associations were also observed in dyads without maternal asthma history, driven by MEP and mono-butyl phthalate (MBP), but not in those with maternal asthma history. We observed protective associations between the phthalate index and respiratory outcomes in analysis of all participants (e.g., ever asthma: AOR; 95% CI: 0.81; 0.68, 0.96), with di(2-ethylhexyl)phthalate (DEHP) metabolites weighted highest.
Results suggest effect modification by child sex and maternal asthma in associations between prenatal phthalate mixtures and child asthma and wheeze.
先前关于产前邻苯二甲酸酯暴露与儿童哮喘的研究结果并不一致。这些研究通常将邻苯二甲酸酯建模为个体而非共同发生的暴露。我们使用混合物方法研究了 ECHO-PATHWAYS 联盟中的两个产前队列的双胞胎:CANDLE 于 2006-2011 年招募,TIDES 于 2011-2013 年招募。父母在孩子 4-6 岁时报告了儿童呼吸道结局:曾患哮喘、当前喘息(过去 12 个月有症状)和当前哮喘(曾患哮喘、最近使用哮喘特定药物治疗和/或当前喘息的两个肯定答复)。我们在第三个孕期尿液中定量了 11 种邻苯二甲酸酯代谢物,并使用加权分位数总和(WQS)逻辑回归来估计与儿童呼吸道结局的关联,使用单独的模型来估计保护和不良关联,调整了协变量。我们检查了儿童性别和母亲哮喘的效应修饰。
在 1481 名女性中,大多数女性为白人(46.6%)或黑人(44.6%);17%的女性报告有哮喘病史。儿童的曾患哮喘、当前喘息和当前哮喘的患病率分别为 12.3%、15.8%和 12.3%。总体而言,与呼吸道结局没有不良关联。在性别分层分析中,男孩的邻苯二甲酸酯指数与所有结局呈负相关(例如,男孩曾患哮喘:WQS 邻苯二甲酸酯指数每增加一个五分位数,调整后的比值比(AOR)为 1.42;95%置信区间(CI)为 1.08,1.85,以单乙基邻苯二甲酸酯(MEP)加权最高)。在没有母亲哮喘史的双胞胎中也观察到不良关联,这主要由 MEP 和单丁基邻苯二甲酸酯(MBP)驱动,但在有母亲哮喘史的双胞胎中则没有。在所有参与者的分析中,我们观察到邻苯二甲酸酯指数与呼吸道结局之间的保护关联(例如,曾患哮喘:AOR;95%CI:0.81;0.68,0.96),以二(2-乙基己基)邻苯二甲酸酯(DEHP)代谢物加权最高。
结果表明,儿童性别和母亲哮喘对产前邻苯二甲酸酯混合物与儿童哮喘和喘息之间的关联有修饰作用。