Fraser Simon Ds, Barker Jenny, Roderick Paul J, Yuen Ho Ming, Shardlow Adam, Morris James E, McIntyre Natasha J, Fluck Richard J, McIntyre Chris W, Taal Maarten W
School of Primary Care, Population Sciences and Medical Education, Faculty of Medicine, University of Southampton, Southampton, UK
School of Primary Care, Population Sciences and Medical Education, Faculty of Medicine, University of Southampton, Southampton, UK.
BMJ Open. 2020 Aug 6;10(8):e040286. doi: 10.1136/bmjopen-2020-040286.
To determine the associations between comorbidities, health-related quality of life (HRQoL) and functional impairment in people with mild-to-moderate chronic kidney disease (CKD) in primary care.
Cross-sectional analysis at 5-year follow-up in a prospective cohort study.
Thirty-two general practitioner surgeries in England.
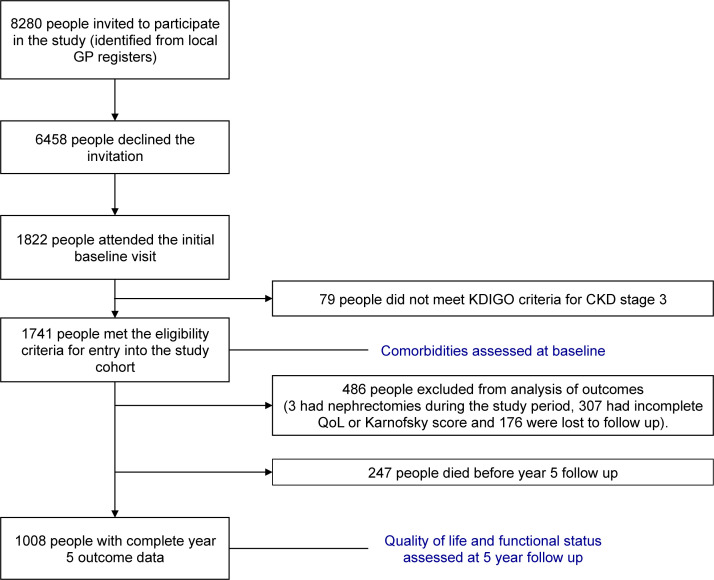
1008 participants with CKD stage 3 (of 1741 people recruited at baseline in the Renal Risk in Derby study) who survived to 5 years and had complete follow-up data for HRQoL and functional status (FS).
HRQoL assessed using the 5-level EQ-5D version (EQ-5D-5L, with domains of mobility, self-care, usual activities, pain/discomfort and anxiety/depression and index value using utility scores calculated from the English general population), and FS using the Karnofsky Performance Status scale (functional impairment defined as Karnofksy score ≤70). Comorbidity was defined by self-reported or doctor-diagnosed condition, disease-specific medication or blood result.
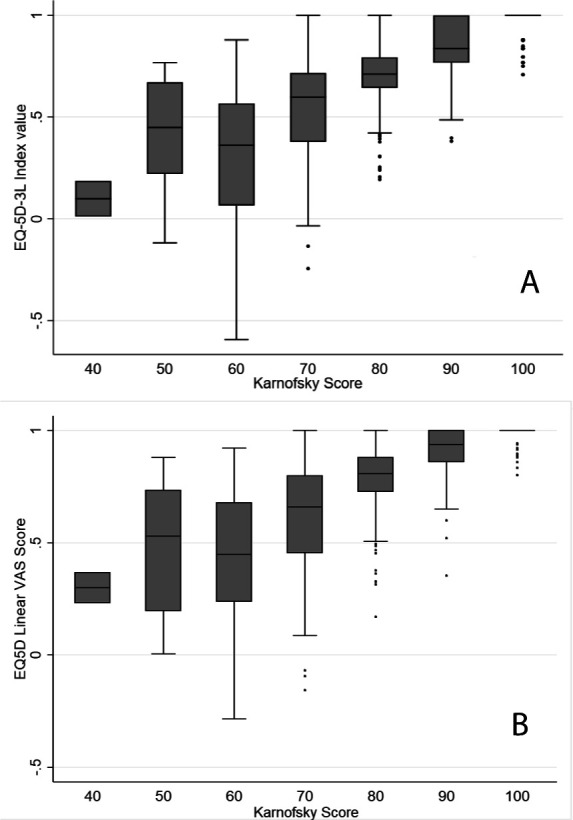
Mean age was 75.8 years. The numbers reporting some problems in EQ-5D-5L domains were: 582 (57.7%) for mobility, 166 (16.5%) for self-care, 466 (46.2%) for usual activities, 712 (70.6%) for pain/discomfort and 319 (31.6%) for anxiety/depression. Only 191 (18.9%) reported no problems in any domain. HRQoL index values showed greater variation among those with lower FS (eg, for those with Karnofsky score of 60, the median (IQR) EQ-5D index value was 0.45 (0.24 to 0.68) compared with 0.94 (0.86 to 1) for those with Karnofsky score of 90). Overall, 234 (23.2%) had functional impairment.In multivariable logistic regression models, functional impairment was independently associated with experiencing problems for all EQ-5D-5L domains (mobility: OR 16.87 (95% CI 8.70 to 32.79, p<0.001, self-care: OR 13.08 (95% CI 8.46 to 20.22), p<0.001, usual activities: OR 8.27 (95% CI 5.43 to 12.58), p<0.001, pain/discomfort: OR 2.94 (95% CI 1.86 to 4.67), p<0.001, anxiety/depression: 3.08 (95% CI 2.23 to 4.27), p<0.001). Higher comorbidity count and obesity were independently associated with problems in mobility, self-care, usual activities and pain/discomfort: for three or more comorbidities versus none: (mobility: OR 2.10 (95% CI 1.08 to 4.10, p for trend 0.002), self-care: OR 2.64 (95% CI 0.72 to 9.67, p for trend 0.05), usual activities: OR 4.20 (95% CI 2.02 to 8.74, p for trend <0.001), pain/discomfort: OR 3.06 (95% CI 1.63 to 5.73, p for trend <0.001)), and for obese (body mass index (BMI) ≥30 kg/m) versus BMI <25 kg/m: (mobility: OR 2.44 (95% CI 1.61 to 3.69, p for trend <0.001), self-care: OR 1.98 (95% CI 1.06 to 3.71, p for trend 0.003), usual activities: OR 1.82 (95% CI 1.19 to 2.76, p for trend 0.019), pain/discomfort: OR 2.37 (95% CI 1.58 to 3.55, p for trend <0.001)). Female sex, lower FS and lower educational attainment were independently associated with anxiety/depression (ORs 1.60 (95% CI 1.18 to 2.16, p 0.002), 3.08 (95% CI 2.23 to 4.27, p<0.001) and 1.67 (95% CI 1.10 to 2.52, p 0.009), respectively). Older age, higher comorbidity count, albuminuria (≥30 mg/mmol vs <3 mg/mmol), lower educational attainment (no formal qualifications vs degree level) and obesity were independently associated with functional impairment (ORs 1.07 (95% CI 1.04 to 1.09, p<0.001), 2.18 (95% CI 0.80 to 5.96, p for trend <0.001), 1.74 (95% CI 0.82 to 3.68, p for trend 0.005), 2.08 (95% CI 1.26 to 3.41, p for trend <0.001) and 4.23 (95% CI 2.48 to 7.20), respectively).
The majority of persons with mild-to-moderate CKD reported reductions in at least one HRQoL domain, which were independently associated with comorbidities, obesity and functional impairment.
National Institute for Health Research Clinical Research Portfolio Study Number 6632.
确定初级保健中轻度至中度慢性肾脏病(CKD)患者的合并症、健康相关生活质量(HRQoL)和功能损害之间的关联。
前瞻性队列研究中5年随访的横断面分析。
英格兰的32家全科医生诊所。
1008名CKD 3期参与者(在德比肾脏风险研究中基线招募的1741人中),存活至5年,并拥有HRQoL和功能状态(FS)的完整随访数据。
使用5级EQ-5D版本评估HRQoL(EQ-5D-5L,包括活动能力、自我护理、日常活动、疼痛/不适和焦虑/抑郁等领域,并使用根据英国普通人群计算的效用得分得出的指数值),使用卡诺夫斯基性能状态量表评估FS(功能损害定义为卡诺夫斯基评分≤70)。合并症由自我报告或医生诊断的疾病、特定疾病药物或血液检查结果定义。
平均年龄为75.8岁。报告在EQ-5D-5L领域存在一些问题的人数分别为:活动能力方面582人(57.7%),自我护理方面166人(16.5%),日常活动方面466人(46.2%),疼痛/不适方面712人(70.6%),焦虑/抑郁方面319人(31.6%)。只有191人(18.9%)报告在任何领域均无问题。HRQoL指数值在FS较低的人群中显示出更大的差异(例如,卡诺夫斯基评分为60的人群,中位数(IQR)EQ-5D指数值为0.45(0.24至0.68),而卡诺夫斯基评分为90的人群为0.94(0.86至1))。总体而言,234人(23.2%)存在功能损害。在多变量逻辑回归模型中,功能损害与所有EQ-5D-5L领域出现问题独立相关(活动能力:比值比(OR)16.87(95%置信区间(CI)8.70至32.79,p<0.001),自我护理:OR 13.08(95% CI 8.46至20.22),p<0.001,日常活动:OR 8.27(95% CI 5.43至12.58),p<0.001,疼痛/不适:OR 2.94(95% CI 1.86至4.67),p<0.001,焦虑/抑郁:3.08(95% CI 2.23至4.27),p<0.001)。更高的合并症计数和肥胖与活动能力、自我护理、日常活动和疼痛/不适方面的问题独立相关:与无合并症相比,有三种或更多合并症:(活动能力:OR 2.10(95% CI 1.08至4.10,趋势p值0.002),自我护理:OR 2.64(95% CI 0.72至9.67,趋势p值0.05),日常活动:OR 4.20(95% CI 2.02至8.74,趋势p值<0.001),疼痛/不适:OR 3.06(95% CI 1.63至5.73,趋势p值<0.001)),以及肥胖(体重指数(BMI)≥30 kg/m²)与BMI<25 kg/m²相比:(活动能力:OR 2.44(95% CI 1.61至3.69,趋势p值<0.001),自我护理:OR 1.98(95% CI 1.06至3.71,趋势p值0.003),日常活动:OR 1.82(95% CI 1.19至2.76,趋势p值0.019),疼痛/不适:OR 2.37(95% CI 1.58至3.55,趋势p值<0.001))。女性、较低的FS和较低的教育程度与焦虑/抑郁独立相关(OR分别为1.60(95% CI 1.18至2.16,p 0.002))、3.08(95% CI 2.23至4.27,p<0.001)和1.67(95% CI 1.10至2.52,p 0.009))。年龄较大、合并症计数较高、蛋白尿(≥30 mg/mmol与<3 mg/mmol)、较低的教育程度(无正规学历与学位水平)和肥胖与功能损害独立相关(OR分别为1.07(95% CI 1.04至1.09,p<0.001)、2.18(95% CI 0.80至5.96,趋势p值<0.001)、1.74(95% CI 0.82至3.68,趋势p值0.005)、2.08(95% CI 1.26至3.41,趋势p值<0.001)和4.23(95% CI 2.48至7.20))。
大多数轻度至中度CKD患者报告至少一个HRQoL领域有所下降,这与合并症、肥胖和功能损害独立相关。
英国国家卫生研究院临床研究组合研究编号6632。