Lumbers Eugenie R, Kandasamy Yoga, Delforce Sarah J, Boyce Amanda C, Gibson Karen J, Pringle Kirsty G
School of Biomedical Sciences and Pharmacy, Faculty of Health and Medicine, The University of Newcastle, Callaghan, NSW, Australia.
Hunter Medical Research Institute, Newcastle, NSW, Australia.
Front Physiol. 2020 Jul 16;11:757. doi: 10.3389/fphys.2020.00757. eCollection 2020.
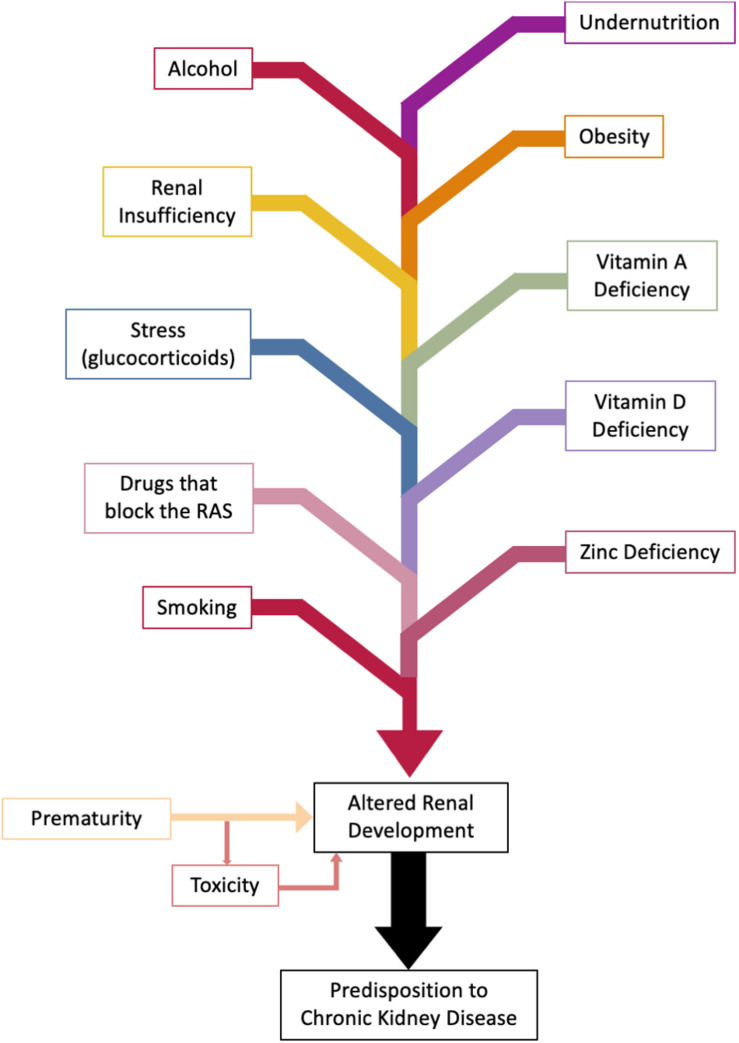
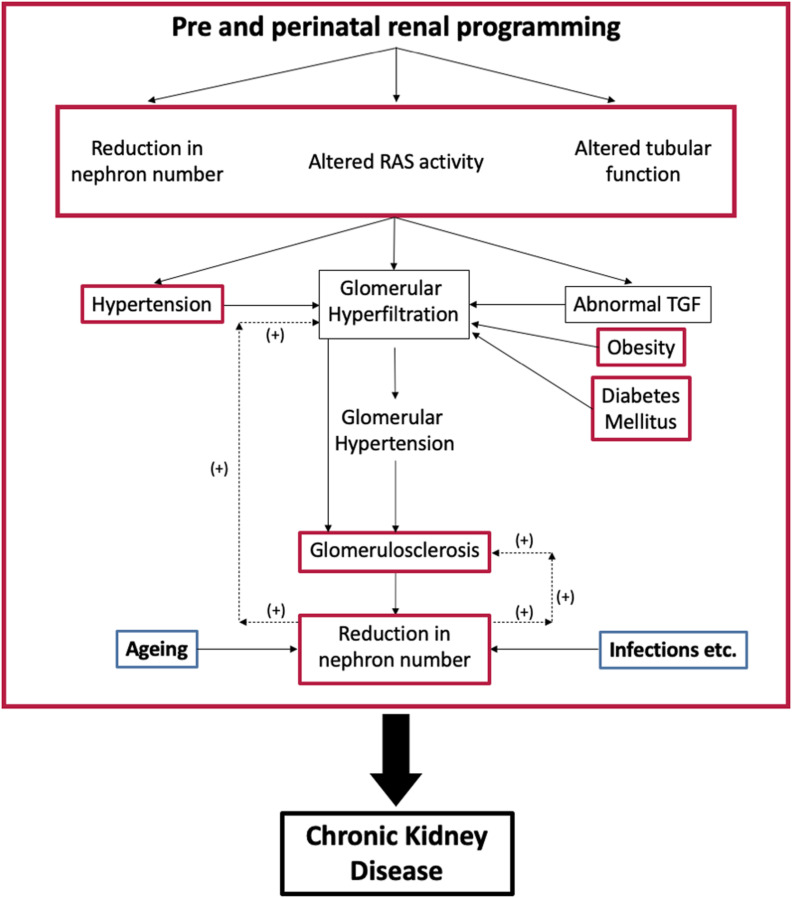
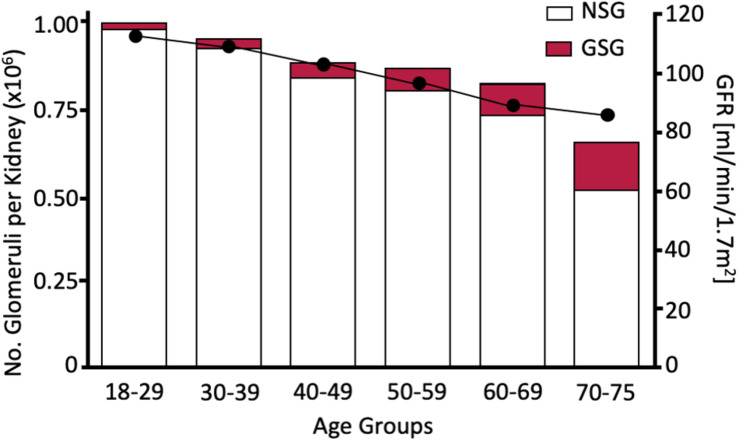
Chronic kidney disease (CKD) can have an insidious onset because there is a gradual decline in nephron number throughout life. There may be no overt symptoms of renal dysfunction until about two thirds or more of the nephrons have been destroyed and glomerular filtration rate (GFR) falls to below 25% of normal (often in mid-late life) (Martinez-Maldonaldo et al., 1992). Once End Stage Renal Disease (ESRD) has been reached, survival depends on renal replacement therapy (RRT). CKD causes hypertension and cardiovascular disease; and hypertension causes CKD. Albuminuria is also a risk factor for cardiovascular disease. The age of onset of CKD is partly determined during fetal life. This review describes the mechanisms underlying the development of CKD in adult life that results from abnormal renal development caused by an adverse intrauterine environment. The basis of this form of CKD is thought to be mainly due to a reduction in the number of nephrons formed which impacts on the age dependent decline in glomerular function. Factors that affect the risk of reduced nephron formation during intrauterine life are discussed and include maternal nutrition (malnutrition and obesity, micronutrients), smoking and alcohol, use of drugs that block the maternal renin-angiotensin system, glucocorticoid excess and maternal renal dysfunction and prematurity. Since CKD, hypertension and cardiovascular disease add to the disease burden in the community we recommend that kidney size at birth should be recorded using ultrasound and those individuals who are born premature or who have small kidneys at this time should be monitored regularly by determining GFR and albumin:creatinine clearance ratio. Furthermore, public health measures aimed at limiting the prevalence of obesity and diabetes mellitus as well as providing advice on limiting the amount of protein ingested during a single meal, because they are all associated with increased glomerular hyperfiltration and subsequent glomerulosclerosis would be beneficial.
慢性肾脏病(CKD)起病隐匿,因为一生中肾单位数量会逐渐减少。在约三分之二或更多肾单位被破坏且肾小球滤过率(GFR)降至正常水平的25%以下(通常在中年后期)之前,可能没有明显的肾功能不全症状(Martinez - Maldonaldo等人,1992年)。一旦达到终末期肾病(ESRD),生存就依赖于肾脏替代治疗(RRT)。CKD会导致高血压和心血管疾病;而高血压也会引发CKD。蛋白尿也是心血管疾病的一个危险因素。CKD的发病年龄部分在胎儿期就已确定。本综述描述了成年期CKD发生发展的机制,其由子宫内不良环境导致的肾脏发育异常引起。这种形式的CKD的基础被认为主要是由于形成的肾单位数量减少,这影响了肾小球功能随年龄的下降。讨论了影响子宫内生活期间肾单位形成减少风险的因素,包括母亲营养(营养不良和肥胖、微量营养素)、吸烟和饮酒、使用阻断母亲肾素 - 血管紧张素系统的药物、糖皮质激素过量、母亲肾功能不全和早产。由于CKD、高血压和心血管疾病增加了社区的疾病负担,我们建议应使用超声记录出生时的肾脏大小,对于早产或此时肾脏较小的个体,应通过测定GFR和白蛋白:肌酐清除率进行定期监测。此外,旨在限制肥胖症和糖尿病患病率的公共卫生措施,以及提供关于限制每餐蛋白质摄入量的建议,因为它们都与肾小球超滤增加及随后的肾小球硬化相关,将是有益的。