Kewan Tariq, Covut Fahrettin, Al-Jaghbeer Mohammed J, Rose Lori, Gopalakrishna K V, Akbik Bassel
Department of Internal Medicine, Cleveland Clinic Fairview Hospital, Cleveland, OH, United States.
Department of Pulmonary and Critical Care Medicine, Cleveland Clinic, Cleveland, OH, United States.
EClinicalMedicine. 2020 Jun 20;24:100418. doi: 10.1016/j.eclinm.2020.100418. eCollection 2020 Jul.
Tocilizumab was approved for chimeric antigen receptor T-cell therapy induced cytokine release syndrome and it may provide clinical benefit for selected COVID-19 patients.
In this retrospective cohort study, we analyzed hypoxic COVID-19 patients who were consecutively admitted between March 13, 2020 and April 19, 2020. Patients with lung infiltrates and elevated inflammatory markers received a single dose of tocilizumab if no contraindication was present. Systemic steroid, hydroxychloroquine, and azithromycin were concomitantly used for majority of the patients.
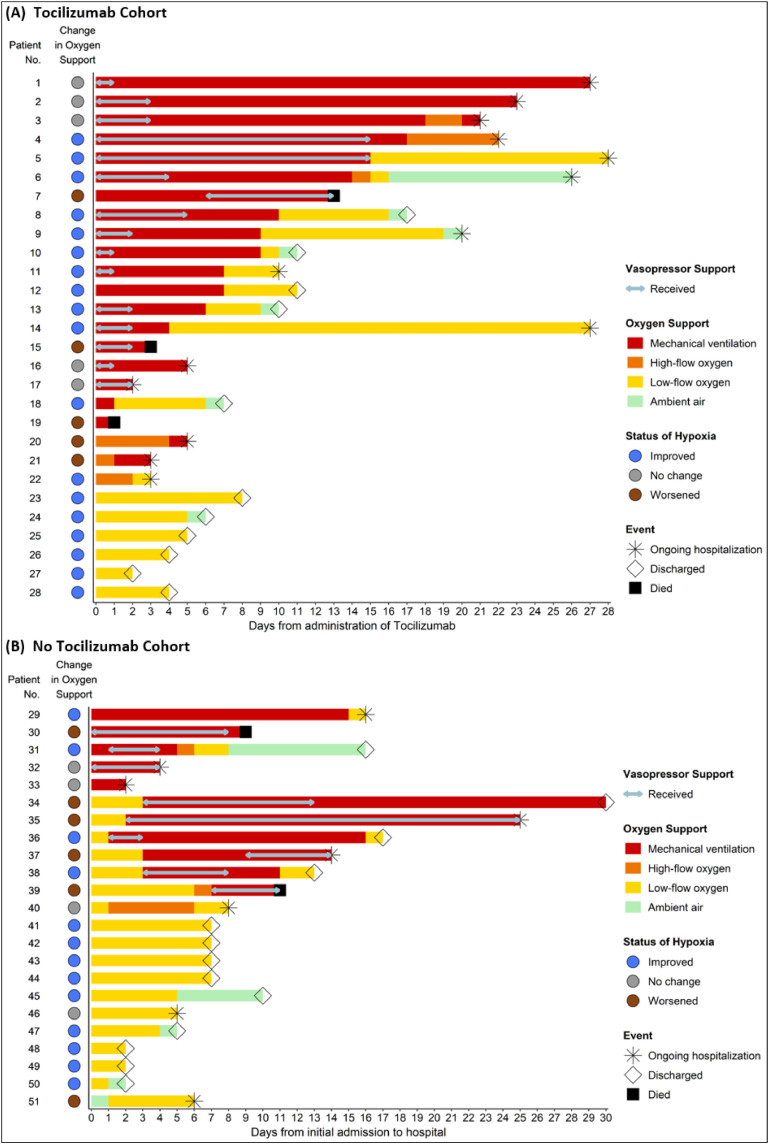
Of the 51 patients included for analysis, 28 (55%) received tocilizumab and 23 (45%) did not receive tocilizumab. Tocilizumab cohort required more invasive ventilation (68% vs. 22%) at baseline and during entire hospitalization (75% vs. 48%). The median time to clinical improvement in tocilizumab vs. no tocilizumab cohorts was 8 days (Interquartile range [IQR]: 6·25 - 9·75 days) vs. 13 days (IQR: 9·75 - 15·25 days) among patients who required mechanical ventilation at any time (Hazard ratio for clinical improvement: 1·83, 95% confidence interval [CI]: 0·57 - 5·84) and 6·5 days vs. 7 days among all patients (Hazard ratio for clinical improvement: 1·14, 95% CI: 0·55 - 2·38), respectively. The median duration of vasopressor support and invasive mechanical ventilation were 2 days (IQR: 1·75 - 4·25 days) vs. 5 days (IQR: 4 - 8 days), = 0.039, and 7 days (IQR: 4 - 14 days) vs. 10 days (IQR: 5 - 15 days) in tocilizumab vs. no tocilizumab cohorts, = 0.11, respectively. Similar rates of hospital-acquired infections occurred in both cohorts (18% in tocilizumab and 22% in no tocilizumab cohort).
In patients with severe COVID-19, tocilizumab was associated with significantly shorter duration of vasopressor support. Although not statistically significant, tocilizumab also resulted in shorter median time to clinical improvement and shorter duration of invasive ventilation. These findings require validation from ongoing clinical trials of Tocilizumab in COVID-19 patients.
托珠单抗已被批准用于治疗嵌合抗原受体T细胞疗法诱导的细胞因子释放综合征,它可能为部分新型冠状病毒肺炎(COVID-19)患者带来临床益处。
在这项回顾性队列研究中,我们分析了2020年3月13日至2020年4月19日期间连续入院的低氧血症COVID-19患者。肺部有浸润且炎症标志物升高的患者,若不存在禁忌证,则接受单剂量托珠单抗治疗。大多数患者同时使用了全身性类固醇、羟氯喹和阿奇霉素。
纳入分析的51例患者中,28例(55%)接受了托珠单抗治疗,23例(45%)未接受托珠单抗治疗。托珠单抗治疗组在基线时和整个住院期间需要有创通气的比例更高(分别为68%对22%和75%对48%)。在任何时候需要机械通气的患者中,托珠单抗治疗组与未接受托珠单抗治疗组临床改善的中位时间分别为8天(四分位间距[IQR]:6.25 - 9.75天)对13天(IQR:9.75 - 15.25天)(临床改善的风险比:1.83,95%置信区间[CI]:0.57 - 5.84),在所有患者中分别为6.5天对7天(临床改善的风险比:1.14,95%CI:0.55 - 2.38)。托珠单抗治疗组与未接受托珠单抗治疗组血管活性药物支持的中位持续时间分别为2天(IQR:1.75 - 4.25天)对5天(IQR:4 - 8天),P = 0.039,有创机械通气的中位持续时间分别为7天(IQR:4 - 14天)对10天(IQR:5 - 15天),P = 0.11。两组医院获得性感染发生率相似(托珠单抗治疗组为18%,未接受托珠单抗治疗组为22%)。
在重症COVID-19患者中,托珠单抗与血管活性药物支持的持续时间显著缩短相关。尽管未达到统计学显著性,但托珠单抗也使临床改善的中位时间缩短,有创通气的持续时间缩短。这些发现需要在托珠单抗治疗COVID-19患者的正在进行的临床试验中得到验证。