Stem Cell Group, UCL Cancer Institute, University College London, London, WC1E 6BT, UK; Manual Blood Sciences, Health Services Laboratories, The Halo Building, 1 Mabledon Place, London WC1H 9AX, UK.
Department of Microbiology, UCLH NHS Hospitals NHS Foundation Trust, 250 Euston Road, London NW1 2PG, UK.
Int J Infect Dis. 2020 Oct;99:381-385. doi: 10.1016/j.ijid.2020.08.004. Epub 2020 Aug 6.
The reasons why some patients with COVID-19 develop pneumonia and others do not are unclear. To better understand this, we used multiparameter flow cytometry to profile circulating leukocytes from non-immunocompromised adult patients with PCR-proven COVID-19 and specifically compared those with mild symptoms with those who had developed pneumonia.
Using clinically validated antibody panels we studied leukocytes from 29 patients with PCR-proven COVID-19. Ten were hypoxic requiring ventilatory support, eleven were febrile but otherwise well, and eight were convalescing having previously required ventilatory support. Additionally, we analysed patients who did not have COVID-19 but received ventilatory support for other reasons. We examined routine Full Blood Count (FBC) specimens that were surplus to routine diagnostic requirements; normal ranges were established in a historic group of healthy volunteers.
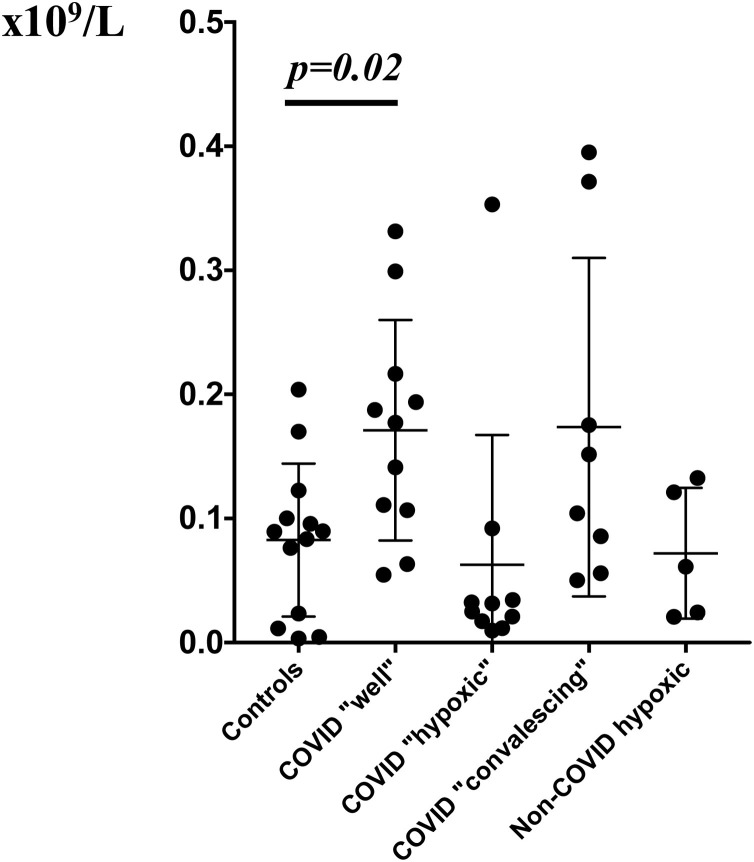
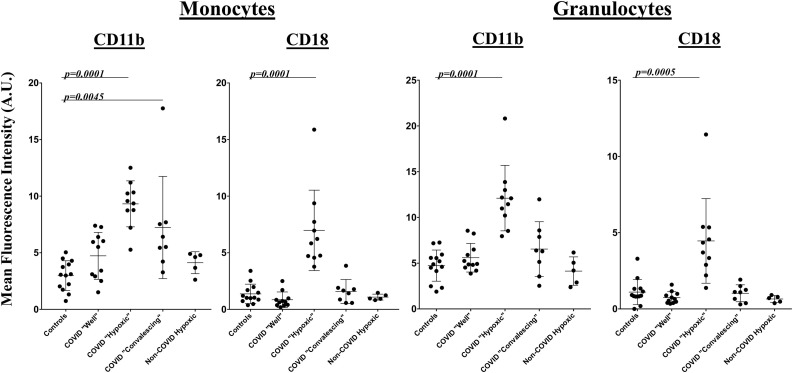
We observed striking and unexpected differences in cells of the innate immune system. Levels of CD11b and CD18, which together comprise Complement Receptor 3 (CR3), were increased in granulocytes and monocytes from hypoxic COVID-19 patients, but not in those with COVID-19 who remained well, or in those without COVID-19 but ventilated for other reasons. Granulocyte and monocyte numbers were unchanged, however Natural Killer (NK) cell numbers were two-fold higher than normal in COVID-19 patients who remained well.
CR3 is central to leukocyte activation and subsequent cytokine release in response to infection. It is also a fibrinogen receptor, and its over-expression in granulocytes and monocytes of patients with respiratory failure tables it as a candidate effector of both the thrombotic and inflammatory features of COVID-19 pneumonia, and both a biomarker of impending respiratory failure and potential therapeutic target. NK cells are innate immune cells that retain immunological memory. Rapid expansion of memory NK cells targeting common antigens shared with other Coronaviruses may explain why most patients with COVID-19 do not develop respiratory complications. Understanding the innate immune response to SARS-CoV-may uncover why most infected individuals experience mild symptoms, and inform a preventive approach to COVID-19 pneumonia in the future.
为什么有些 COVID-19 患者会发展为肺炎,而有些患者则不会,原因尚不清楚。为了更好地了解这一点,我们使用多参数流式细胞术对经 PCR 证实的 COVID-19 非免疫功能低下成年患者的循环白细胞进行了分析,并特别比较了轻症患者和发生肺炎的患者。
我们使用经过临床验证的抗体面板研究了 29 例经 PCR 证实的 COVID-19 患者的白细胞。其中 10 例为低氧血症需要通气支持,11 例为发热但其他情况良好,8 例为先前需要通气支持的恢复期患者。此外,我们还分析了因其他原因接受通气支持但未感染 COVID-19 的患者。我们检查了常规全血细胞计数 (FBC) 标本,这些标本是常规诊断要求之外的剩余标本;在一组健康志愿者中建立了正常范围。
我们观察到先天免疫系统细胞的惊人且出乎意料的差异。在缺氧 COVID-19 患者的粒细胞和单核细胞中,CD11b 和 CD18 的水平(共同构成补体受体 3 [CR3])升高,但在病情良好的 COVID-19 患者中没有升高,也不在因其他原因而接受通气支持但未感染 COVID-19 的患者中升高。粒细胞和单核细胞数量没有变化,但病情良好的 COVID-19 患者的自然杀伤 (NK) 细胞数量是正常的两倍。
CR3 是白细胞激活和随后对感染释放细胞因子的核心。它也是纤维蛋白原受体,其在呼吸衰竭患者的粒细胞和单核细胞中的过度表达表明它是 COVID-19 肺炎的血栓形成和炎症特征的候选效应物,也是呼吸衰竭即将发生的生物标志物和潜在的治疗靶点。NK 细胞是具有免疫记忆的先天免疫细胞。针对与其他冠状病毒共享的常见抗原的记忆 NK 细胞的快速扩增可能解释了为什么大多数 COVID-19 患者不会出现呼吸并发症。了解对 SARS-CoV 的先天免疫反应可能揭示为什么大多数感染个体症状较轻,并为未来 COVID-19 肺炎提供预防方法。