Department of Surgery, National Yang-Ming University Hospital, Yilan, Taiwan, ROC.
School of Medicine, National Yang-Ming University, Taipei, Taiwan, ROC.
J Chin Med Assoc. 2020 Oct;83(10):911-917. doi: 10.1097/JCMA.0000000000000398.
Most clinical guidelines recommend measuring postoperative carcinoembryonic antigen (CEA) levels to predict the prognosis of colorectal cancer. However, type II diabetes can increase serum CEA levels which may bias the prognosis. Thus, we aimed to evaluate the impact of type II diabetes on CEA prognostic accuracy in colorectal cancer.
This retrospective cohort study included 407 patients who underwent curative resection for stage I to III colorectal adenocarcinoma in a single institution between January 2010 and June 2018. The patients were categorized into two groups according to their postoperative serum CEA levels: group A <5.0 ng/mL (n = 341) and group B ≥5.0 ng/mL (n = 66). Patients were also categorized into two subgroups according to their history of type II diabetes: patients with type II diabetes mellitus (n = 112) and patients without type II diabetes (n = 295).
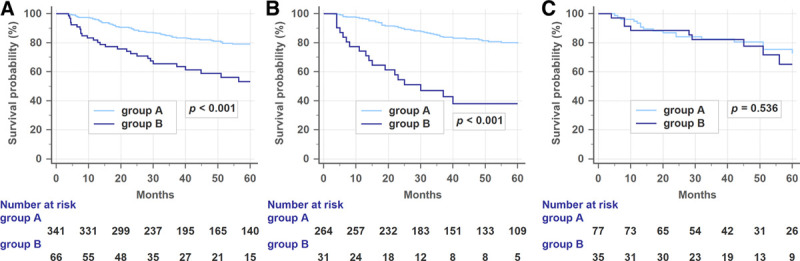
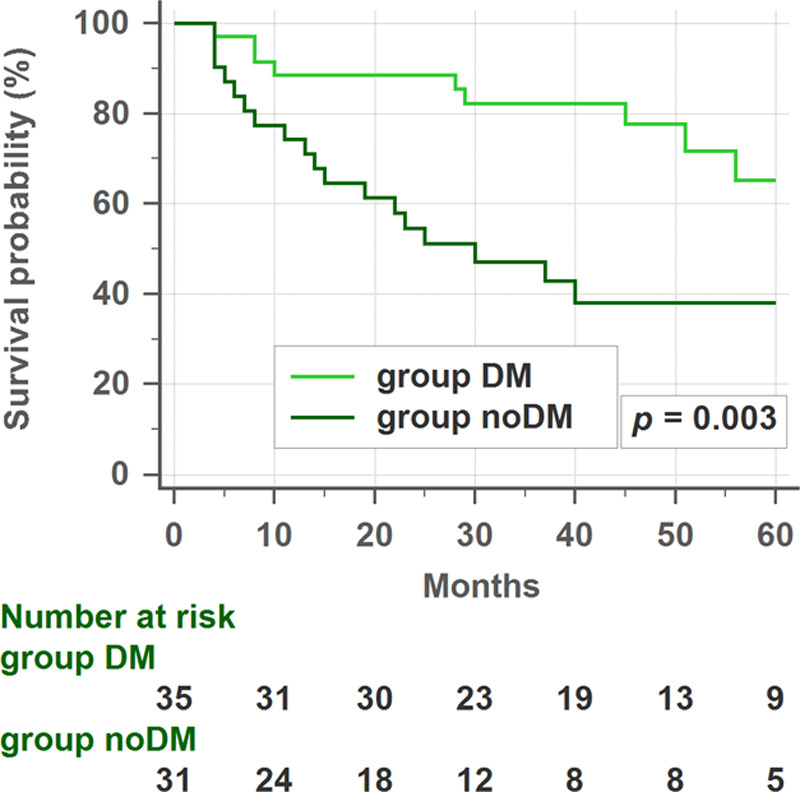
The 3-year disease-free survival (DFS) rates were significantly higher in patients with normal postoperative CEA (group A, 83.8%) than in patients with elevated preoperative and postoperative CEA (group B, 63.6%) (p < 0.001). However, although patients with type II diabetes mellitus had higher postoperative CEA levels than those without type II diabetes mellitus (3.1 vs 2.5 ng/mL, p < 0.001), group B patients with type II diabetes mellitus had a significantly higher 3-year DFS rate than those without type II diabetes mellitus (80.0% vs 55.6%, p = 0.003).
Type II diabetes was associated with higher preoperative and postoperative CEA levels in patients with colorectal cancer. Consequently, elevated postoperative CEA level was not associated with shorter 3-year DFS in patients with type II diabetes, as opposed to patients without type II diabetes. Therefore, colorectal cancer patients with type II diabetes may need alternative tumor markers to be used during the surveillance strategy after curative surgery.
大多数临床指南建议测量术后癌胚抗原(CEA)水平以预测结直肠癌的预后。然而,2 型糖尿病会升高血清 CEA 水平,从而可能影响预后的判断。因此,我们旨在评估 2 型糖尿病对结直肠癌患者 CEA 预后准确性的影响。
这是一项回顾性队列研究,纳入了 2010 年 1 月至 2018 年 6 月在一家医疗机构接受根治性切除术治疗 I 期至 III 期结直肠腺癌的 407 例患者。根据术后血清 CEA 水平将患者分为两组:组 A <5.0ng/mL(n = 341)和组 B ≥5.0ng/mL(n = 66)。根据患者是否患有 2 型糖尿病,将患者进一步分为两组:患有 2 型糖尿病的患者(n = 112)和未患 2 型糖尿病的患者(n = 295)。
术后 CEA 正常(组 A,83.8%)的患者 3 年无病生存率(DFS)明显高于术后 CEA 升高的患者(组 B,63.6%)(p < 0.001)。然而,尽管患有 2 型糖尿病的患者术后 CEA 水平高于未患 2 型糖尿病的患者(3.1 与 2.5ng/mL,p < 0.001),但组 B 中有 2 型糖尿病的患者 3 年 DFS 率明显高于未患 2 型糖尿病的患者(80.0%与 55.6%,p = 0.003)。
2 型糖尿病与结直肠癌患者术前和术后 CEA 水平升高有关。因此,在患有 2 型糖尿病的患者中,术后 CEA 水平升高与 3 年 DFS 无显著相关性,而在未患有 2 型糖尿病的患者中则呈负相关。因此,结直肠癌合并 2 型糖尿病的患者在接受根治性手术后的监测策略中可能需要使用其他肿瘤标志物。