Kings Health Economics, Institute of Psychiatry Psychology and Neuroscience, Kings College London, London, United Kingdom.
King's Technology Evaluation Centre, School of Biomedical Engineering & Imaging Sciences, King's College London, London, United Kingdom.
PLoS One. 2020 Aug 10;15(8):e0236783. doi: 10.1371/journal.pone.0236783. eCollection 2020.
Selective dorsal rhizotomy (SDR) has gained interest as an intervention to reduce spasticity and pain, and improve quality of life and mobility in children with cerebral palsy mainly affecting the legs (diplegia). We evaluated the cost-effectiveness of SDR in England.
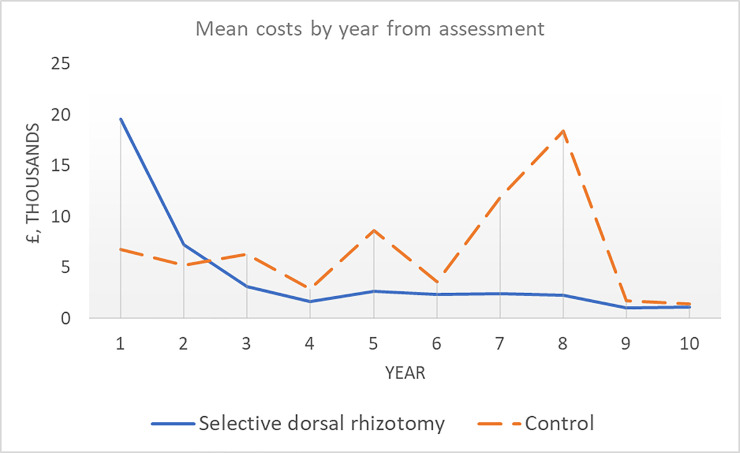
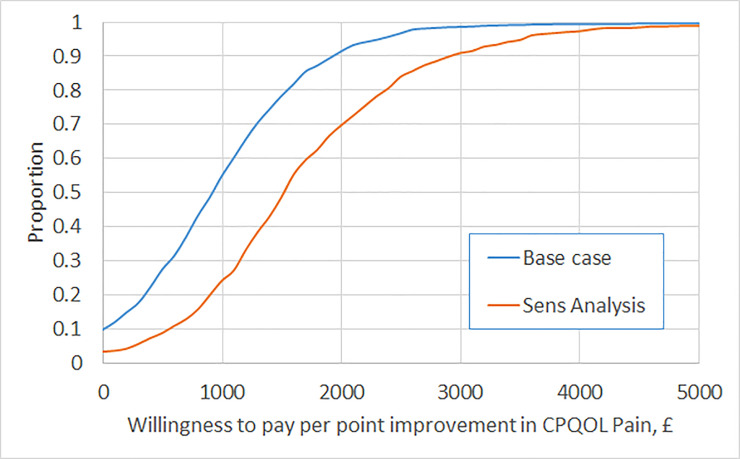
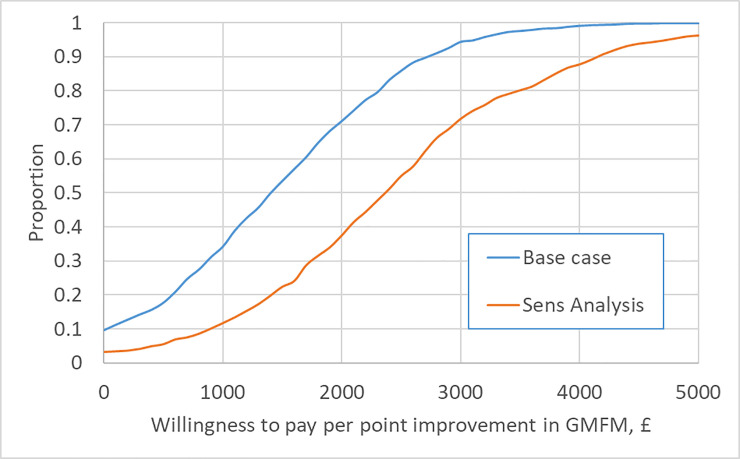
Cost-effectiveness was quantified with respect to Gross Motor Function Measure (GMFM-66) and the pain dimension of the Cerebral Palsy Quality of Life questionnaire for Children (CPQOL-Child). Data on outcomes following SDR over two years were drawn from a national evaluation in England which included 137 children, mean age 6.6 years at surgery. The incremental impact of SDR on GMFM-66 was determined through comparison with data from a historic Canadian cohort not undergoing SDR. Another single centre provided data on hospital care over ten years for 15 children undergoing SDR at a mean age of 7.0 years, and a comparable cohort managed without SDR. The incremental impact of SDR on pain was determined using a before and after comparison using data from the national evaluation. Missing data were imputed using multiple imputation. Incremental costs of SDR were determined as the difference in costs over 5 years for the patients undergoing SDR and those managed without SDR. Uncertainty was quantified using bootstrapping and reported as the cost-effectiveness acceptability curve.
In the base case, the incremental cost-effectiveness ratios (ICERs) for SDR are £1,382 and £903 with respect to a unit improvement in GMFM-66 and the pain dimension of CPQOL-Child, respectively. Inclusion of data to 10 years indicates SDR is cheaper than management without SDR. Incremental costs and ICERs for SDR rose in sensitivity analysis applying an alternative regression model to cost data.
Data on outcomes from a large observational study of SDR and long-term cost data on children who did and did not receive SDR indicates SDR is cost-effective.
选择性脊神经后根切断术(SDR)作为一种干预措施,已引起人们的关注,可减少脑瘫患儿(主要影响腿部)的痉挛、疼痛,提高生活质量和活动能力。我们评估了 SDR 在英国的成本效益。
使用粗大运动功能测量量表(GMFM-66)和脑瘫儿童生活质量问卷(CPQOL-Child)的疼痛维度,从英国全国性评估中获得 SDR 两年后的结果数据,该评估纳入了 137 名儿童,手术时平均年龄为 6.6 岁。SDR 对 GMFM-66 的增量影响通过与未接受 SDR 的加拿大历史队列数据进行比较来确定。另一家单一中心提供了 15 名 7.0 岁接受 SDR 治疗的儿童十年间的住院护理数据,以及未接受 SDR 治疗的可比队列数据。使用全国性评估中的数据,通过前后对比来确定 SDR 对疼痛的增量影响。使用多重插补法填补缺失数据。SDR 的增量成本被确定为接受 SDR 治疗的患者与未接受 SDR 治疗的患者在 5 年内的成本差异。使用自举法量化不确定性,并报告成本效益可接受性曲线。
在基础情况下,SDR 的增量成本效益比(ICER)分别为 1382 英镑和 903 英镑,对应 GMFM-66 增加一个单位和 CPQOL-Child 疼痛维度的改善。纳入到 10 年的数据表明,SDR 的成本低于不接受 SDR 治疗。在对成本数据应用替代回归模型的敏感性分析中,SDR 的增量成本和 ICER 上升。
SDR 的大型观察性研究结果数据和未接受 SDR 治疗的儿童的长期成本数据表明,SDR 具有成本效益。