Chapin Jennifer L, Gray Lauren Tabor, Vasilopoulos Terrie, Anderson Amber, DiBiase Lauren, York Justine Dallal, Robison Raele, Wymer James, Plowman Emily K
Aerodigestive Research Core, University of Florida, Gainesville, FL, United States of America.
Department of Neurology, Phil Smith Neuroscience Institute, Holy Cross Hospital, Fort Lauderdale, FL, United States of America.
PLoS One. 2020 Aug 13;15(8):e0236804. doi: 10.1371/journal.pone.0236804. eCollection 2020.
The ALS Functional Rating Scale-Revised (ALSFRS-R) is the most commonly utilized instrument to index bulbar function in both clinical and research settings. We therefore aimed to evaluate the diagnostic utility of the ALSFRS-R bulbar subscale and swallowing item to detect radiographically confirmed impairments in swallowing safety (penetration or aspiration) and global pharyngeal swallowing function in individuals with ALS.
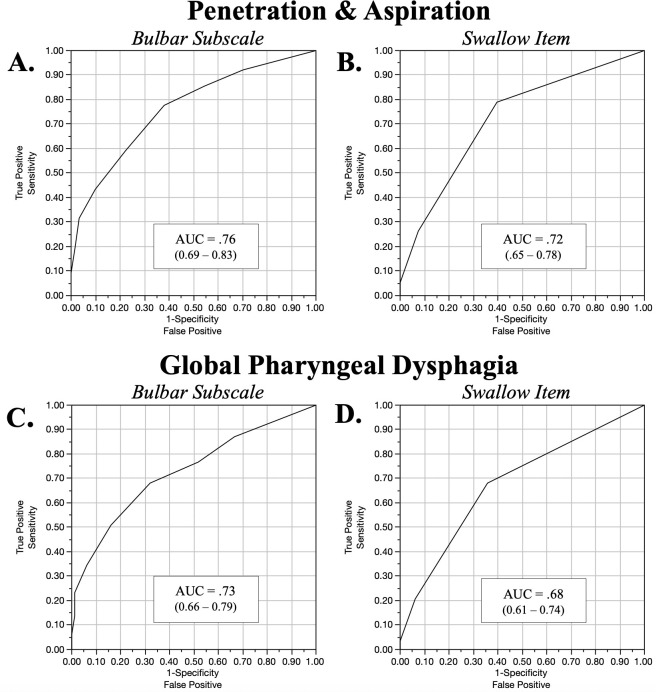
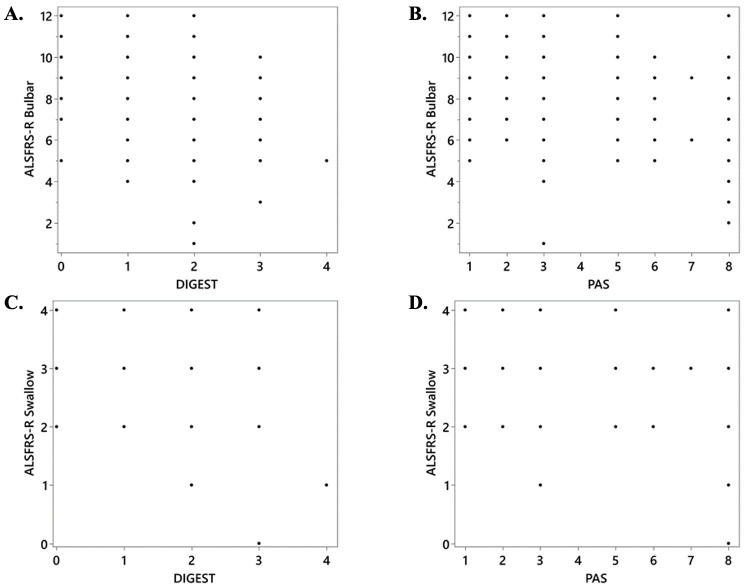
Two-hundred and one individuals with ALS completed the ALSFRS-R and the gold standard videofluoroscopic swallowing exam (VFSE). Validated outcomes including the Penetration-Aspiration Scale (PAS) and Dynamic Imaging Grade of Swallowing Toxicity (DIGEST) were assessed in duplicate by independent and blinded raters. Receiver operator characteristic curve analyses were performed to assess accuracy of the ALSFRS-R bulbar subscale and swallowing item to detect radiographically confirmed unsafe swallowing (PAS > 3) and global pharyngeal dysphagia (DIGEST >1).
Although below acceptable screening tool criterion, a score of ≤ 3 on the ALSFRS-R swallowing item optimized classification accuracy to detect global pharyngeal dysphagia (sensitivity: 68%, specificity: 64%, AUC: 0.68) and penetration/aspiration (sensitivity: 79%, specificity: 60%, AUC: 0.72). Depending on score selection, sensitivity and specificity of the ALSFRS-R bulbar subscale ranged between 34-94%. A score of < 9 optimized classification accuracy to detect global pharyngeal dysphagia (sensitivity: 68%, specificity: 68%, AUC: 0.76) and unsafe swallowing (sensitivity:78%, specificity:62%, AUC: 0.73).
The ALSFRS-R bulbar subscale or swallowing item did not demonstrate adequate diagnostic accuracy to detect radiographically confirmed swallowing impairment. These results suggest the need for alternate screens for dysphagia in ALS.
修订版肌萎缩侧索硬化功能评定量表(ALSFRS-R)是临床和研究中最常用于评估延髓功能的工具。因此,我们旨在评估ALSFRS-R延髓亚量表和吞咽项目对检测肌萎缩侧索硬化患者经影像学证实的吞咽安全性损害(穿透或误吸)及整体咽部吞咽功能的诊断效用。
201例肌萎缩侧索硬化患者完成了ALSFRS-R和金标准视频荧光吞咽检查(VFSE)。由独立且不知情的评估者对包括穿透-误吸量表(PAS)和吞咽毒性动态成像分级(DIGEST)在内的验证结果进行了两次评估。进行了受试者操作特征曲线分析,以评估ALSFRS-R延髓亚量表和吞咽项目检测经影像学证实的不安全吞咽(PAS>3)和整体咽部吞咽困难(DIGEST>1)的准确性。
尽管低于可接受的筛查工具标准,但ALSFRS-R吞咽项目得分≤3可优化检测整体咽部吞咽困难的分类准确性(敏感性:68%,特异性:64%,曲线下面积:0.68)和穿透/误吸(敏感性:79%,特异性:60%,曲线下面积:0.72)。根据得分选择,ALSFRS-R延髓亚量表的敏感性和特异性在34%-94%之间。得分<9可优化检测整体咽部吞咽困难(敏感性:68%,特异性:68%,曲线下面积:0.76)和不安全吞咽(敏感性:78%,特异性:62%,曲线下面积:0.73)的分类准确性。
ALSFRS-R延髓亚量表或吞咽项目在检测经影像学证实的吞咽损害方面未显示出足够的诊断准确性。这些结果表明,肌萎缩侧索硬化患者的吞咽困难需要其他筛查方法。