Beer-Furlan André, Priddy Blake H, Jamshidi Ali O, Shaikhouni Ammar, Prevedello Luciano M, Ditzel Filho Leo, Otto Bradley A, Carrau Ricardo L, Prevedello Daniel M
Department of Neurological Surgery, Rush University Medical Center, Chicago, IL, United States.
Department of Neurological Surgery, Wexner Medical Center, The Ohio State University College of Medicine, Columbus, OH, United States.
Front Neurol. 2020 Jul 24;11:652. doi: 10.3389/fneur.2020.00652. eCollection 2020.
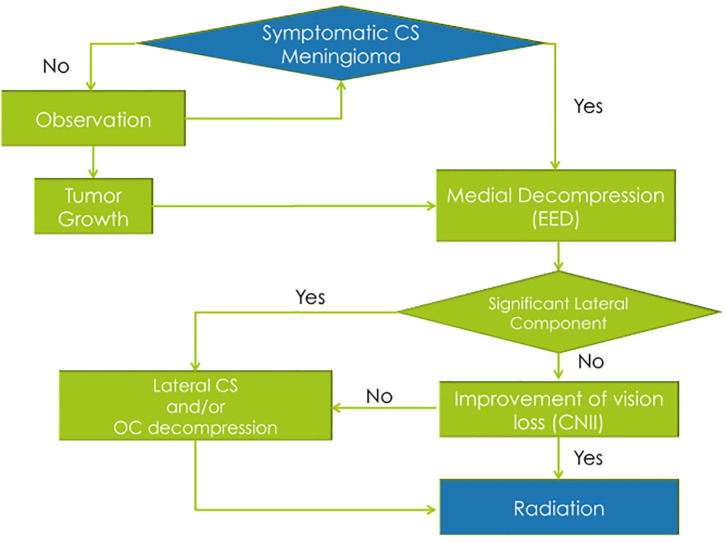
The efficacy and safety of radiosurgery led to paradigm shift in the management of cavernous sinus meningiomas. Nevertheless, patients are still significantly affected by cranial nerve deficits related to the mass effect of these tumors. Our management strategy involves the combination of a functional surgical decompression followed by radiation therapy. We reviewed a single institution's cohort of patients who underwent endoscopic endonasal decompression (EED) for symptomatic meningiomas primarily involving the cavernous sinus (CS) from 2010 to 2016. The preoperative neuro-ophthalmological exam was compared to the 1- and 6-month postoperative exams. The patient's length of hospital stay, complications, and radiological and clinical follow-up were noted. A total of 17 patients underwent EED for CS meningiomas that fit our radiological criteria. The final outcome at the 6-month visit showed five patients (62.5%) with normalization of deficit and three patients (37.5%) with partial improvement of the CNII deficit. Out of the 12 patients who had cavernous sinus cranial nerves (CSCN) deficits, the final outcome at the 6-month visit showed four patients (33.33%) with normalization of deficit, seven patients (58.3%) with partial improvement, and one patient (8.33%) with no improvement. There were no intraoperative complications. The EED for CS meningiomas is a valuable technique when addressing acute/subacute CNII and CSCN deficits. This conservative surgical approach showed good functional outcomes, low morbidity, and low complication rates. However, it does not exempt the need for radiosurgery/radiation therapy for control of tumor growth.
放射外科手术的有效性和安全性导致了海绵窦脑膜瘤治疗模式的转变。然而,患者仍受到与这些肿瘤占位效应相关的颅神经功能缺损的显著影响。我们的治疗策略包括功能性手术减压联合放射治疗。我们回顾了一家机构中2010年至2016年因主要累及海绵窦(CS)的有症状脑膜瘤而接受鼻内镜下经鼻减压术(EED)的患者队列。将术前神经眼科检查结果与术后1个月和6个月的检查结果进行比较。记录患者的住院时间、并发症以及影像学和临床随访情况。共有17例患者因符合我们放射学标准的海绵窦脑膜瘤接受了EED。6个月随访时的最终结果显示,5例患者(62.5%)功能缺损恢复正常,3例患者(37.5%)动眼神经(CNII)功能缺损部分改善。在12例有海绵窦颅神经(CSCN)功能缺损的患者中,6个月随访时的最终结果显示,4例患者(33.33%)功能缺损恢复正常,7例患者(58.3%)部分改善,1例患者(8.33%)无改善。术中无并发症。对于处理急性/亚急性CNII和CSCN功能缺损,EED治疗海绵窦脑膜瘤是一项有价值的技术。这种保守的手术方法显示出良好的功能结果、低发病率和低并发症发生率。然而,它并不能免除为控制肿瘤生长而进行放射外科手术/放射治疗的必要性。