Department of Interventional Neuroradiology, Beijing Tiantan Hospital, Capital Medical University, Beijing, People's Republic of China.
China National Clinical Research Center for Neurological Diseases, Beijing, People's Republic of China.
Clin Interv Aging. 2020 Jul 23;15:1241-1248. doi: 10.2147/CIA.S238769. eCollection 2020.
Whether tirofiban is safe and effective for acute ischemic stroke (AIS) patients undergoing mechanical thrombectomy (MT) with preceding intravenous thrombolysis (IVT) remains unclear. We aim to evaluate the safety and efficacy of tirofiban during MT for patients with preceding IVT.
Patients who underwent MT and preceding IVT were derived from the ANGEL registry and were dichotomized into tirofiban and non-tirofiban group according to whether rescue tirofiban was performed. The safety endpoints were sICH, total ICH and distal embolization. The efficacy endpoints were arterial recanalization, three-month functional independence (modified Rankin Scale [mRS]: 0-2) and mortality.
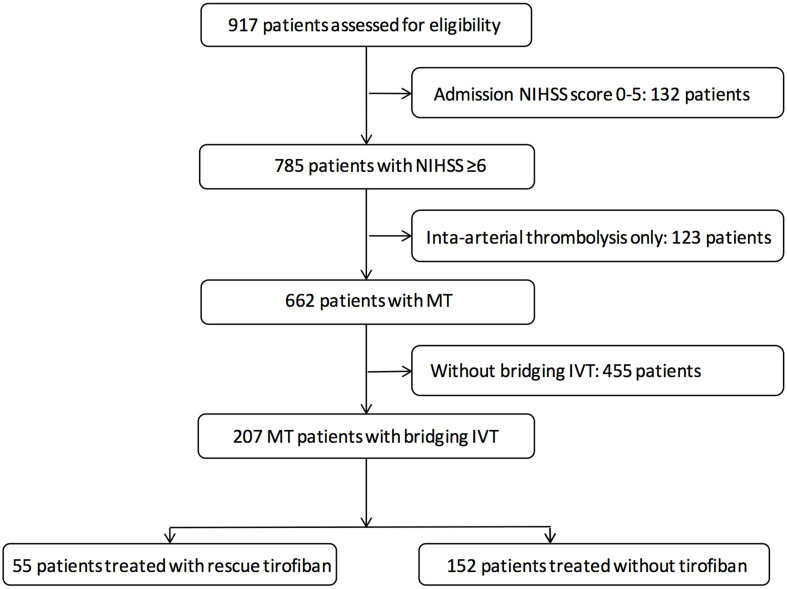
We included 207 MT patients with preceding IVT from the entire registry. Among them, there were 55 in tirofiban group and 152 in non-tirofiban group, and 17 (8.2%) patients suffered sICH and 36 (17.4%) suffered ICH within 24 hours post-MT; 11 (5.3%) distal embolization of thrombus; 111 (53.6%) achieved functional independence and 34 (16.4%) died after three-month follow-up. No significant differences in safety outcomes on sICH, ICH and distal embolization of thrombus and efficacy outcomes on recanalization and long-term functional independence were found between tirofiban and non-tirofiban group for the entire cohort (p>0.05 for all groups). Tirofiban was correlated with long-term mortality reduction for patients underwent MT and preceding IVT (adjusted hazard ratio 0.28 [0.08-0.94], adjusted p=0.03).
In AIS patients who underwent MT and preceding IVT, rescue tirofiban was not correlated with increased risk of safety endpoints on sICH, ICH or distal embolization of thrombus, and might be associated with a lower risk of long-term mortality. Further study is needed to confirm the effect of early antiplatelet therapy with tirofiban for patients underwent MT and preceding IVT.
替罗非班在接受静脉溶栓(IVT)前进行机械取栓(MT)的急性缺血性卒中(AIS)患者中是否安全有效尚不清楚。我们旨在评估 MT 期间替罗非班在接受 IVT 前的安全性和疗效。
来自 ANGEL 登记处的接受 MT 并接受 IVT 的患者被分为替罗非班组和非替罗非班组,根据是否进行挽救性替罗非班治疗进行分组。安全性终点为 sICH、总 ICH 和远端栓塞。有效性终点为动脉再通、3 个月功能独立性(改良 Rankin 量表 [mRS]:0-2)和死亡率。
我们从整个登记处纳入了 207 例接受 IVT 前的 MT 患者。其中,替罗非班组 55 例,非替罗非班组 152 例,17 例(8.2%)患者在 MT 后 24 小时内发生 sICH,36 例(17.4%)发生 24 小时内 ICH;11 例(5.3%)发生血栓远端栓塞;111 例(53.6%)实现功能独立性,34 例(16.4%)在 3 个月随访时死亡。替罗非班组和非替罗非班组在整个队列的安全性结局(sICH、ICH 和血栓远端栓塞)和有效性结局(再通和长期功能独立性)方面均无显著差异(所有组 p>0.05)。替罗非班与接受 MT 和 IVT 的患者的长期死亡率降低相关(调整后的危险比 0.28 [0.08-0.94],调整后的 p=0.03)。
在接受 MT 和 IVT 的 AIS 患者中,挽救性替罗非班与 sICH、ICH 或血栓远端栓塞等安全性终点的风险增加无关,并且可能与长期死亡率降低相关。需要进一步的研究来确认替罗非班在接受 MT 和 IVT 前的早期抗血小板治疗的效果。