Danckert Bolette, Horsbøl Trine Allerslev, Andersen Ole, Dalton Susanne Oksbjerg, Christensen Jane, Rasted Margit, Petersen Astrid, Nørgaard Mette, Azawi Nessn, Lund Lars, Donskov Frede
Director´s Office, Danish Cancer Society Research Center, Copenhagen, Denmark.
Survivorship and Inequality in Cancer, Danish Cancer Society Research Center, Copenhagen, Denmark.
Clin Epidemiol. 2020 Jul 27;12:807-814. doi: 10.2147/CLEP.S258755. eCollection 2020.
The Danish multidisciplinary renal cancer group (DaRenCa) established the nationwide database DaRenCaData in 2010. The Danish Cancer Registry (DCR) has been considered the golden standard. In contrast to DCR, DaRenCaData required the diagnosis to be histologically or cytologically verified. DaRenCaData and DCR have not previously been compared.
We included patients with renal cell carcinoma registered in DaRenCaData and/or DCR from August 1st 2010 to December 31st 2015. We computed completeness and positive predictive value (PPV) of a diagnosis in DaRenCaData compared with DCR, 1-year, 3-year and 5-year mortality rate ratios, and relative survival.
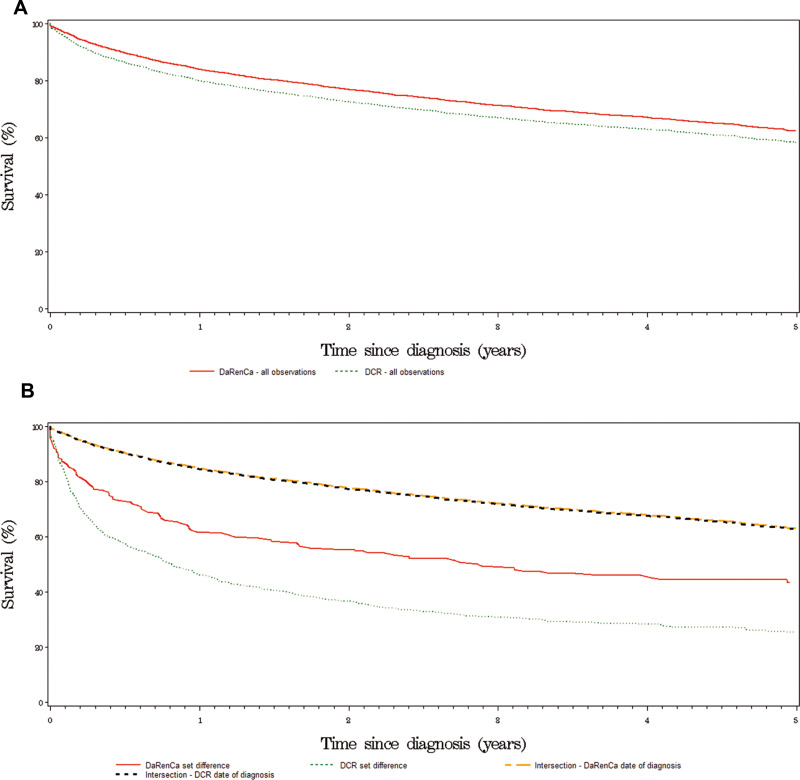
We identified 4890 patients in the two registries. Of these, 4326 were registered in DaRenCaData and 4714 in DCR. Completeness of DaRenCaData was 88% [95% CI, 87-89%] and increased during the period from 82% to 94%. The PPV was 96% [95% CI, 95-97%]. A total of 4150 patients (85%) were found in both registries, 4% (176 patients) in DaRenCaData only, and 12% (564 patients) in DCR only. The relative survival was higher for patients in DaRenCaData vs DCR; the 1-year and 5-year relative survival was 85% vs 81% and 65% vs 59%, respectively. Compared with patients registered in both registries, the mortality rates were higher in patients registered in DaRenCaData only (1-year hazard ratio (HR)=2.84 [95% CI, 2.20-3.68]) or DCR only (1-year HR=4.29 [95% CI, 3.72-4.93]). Observed in both registries, survival improved over time with a 7% yearly reduction in death based on estimations of 1-year mortality rate ratios.
DaRenCaData had high and increasing completeness and high PPV, establishing it as a high-quality research database. Observed in both registries, renal cell carcinoma mortality declined over time; patients only registered in DCR or DaRenCaData had poorer outcomes. This study points to the importance of assessing the inclusion criteria when interpreting registry-based studies.
丹麦多学科肾癌研究小组(DaRenCa)于2010年建立了全国性数据库DaRenCaData。丹麦癌症登记处(DCR)一直被视为金标准。与DCR不同,DaRenCaData要求诊断需经组织学或细胞学验证。此前尚未对DaRenCaData和DCR进行比较。
我们纳入了2010年8月1日至2015年12月31日在DaRenCaData和/或DCR中登记的肾细胞癌患者。我们计算了与DCR相比,DaRenCaData中诊断的完整性和阳性预测值(PPV)、1年、3年和5年死亡率比值以及相对生存率。
我们在两个登记处共识别出4890名患者。其中,4326名在DaRenCaData中登记,4714名在DCR中登记。DaRenCaData的完整性为88%[95%置信区间,87 - 89%],且在此期间从82%增至94%。PPV为96%[95%置信区间,95 - 97%]。两个登记处共发现4150名患者(85%),仅在DaRenCaData中发现4%(176名患者),仅在DCR中发现12%(564名患者)。DaRenCaData患者的相对生存率高于DCR患者;1年和5年相对生存率分别为85%对81%以及65%对59%。与在两个登记处均登记的患者相比,仅在DaRenCaData中登记的患者(1年风险比(HR)=2.84[95%置信区间,2.20 - 3.68])或仅在DCR中登记的患者(1年HR = 4.29[95%置信区间,3.72 - 4.93])的死亡率更高。在两个登记处均观察到,基于1年死亡率比值估计,生存率随时间推移有所改善,每年死亡风险降低7%。
DaRenCaData具有较高且不断提高的完整性以及较高的PPV,使其成为一个高质量的研究数据库。在两个登记处均观察到,肾细胞癌死亡率随时间下降;仅在DCR或DaRenCaData中登记的患者预后较差。本研究指出在解释基于登记处的研究时评估纳入标准的重要性。