Zhang Hongxia, Guang Yang, He Wen, Cheng Linggang, Yu Tengfei, Tang Yu, Song Haiman, Liu Xin, Zhang Yukang
Department of Ultrasound, Beijing Tiantan Hospital, Capital Medical University, Beijing, China.
J Thorac Dis. 2020 Jul;12(7):3697-3705. doi: 10.21037/jtd-2019-abc-03.
To investigate puncture skills and complications prevention in ultrasound-guided percutaneous needle biopsy for peripheral lung lesions.
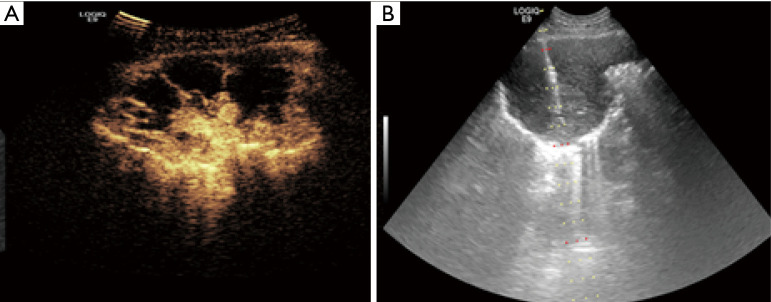
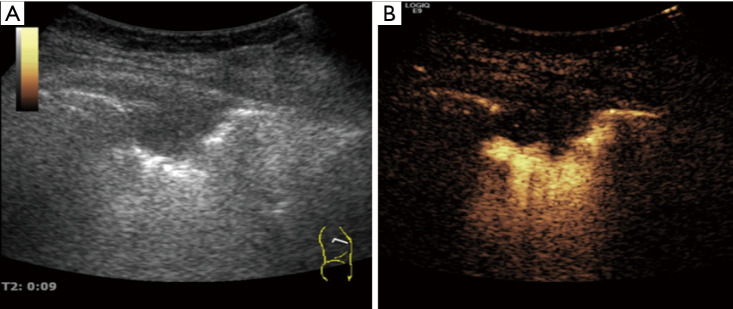
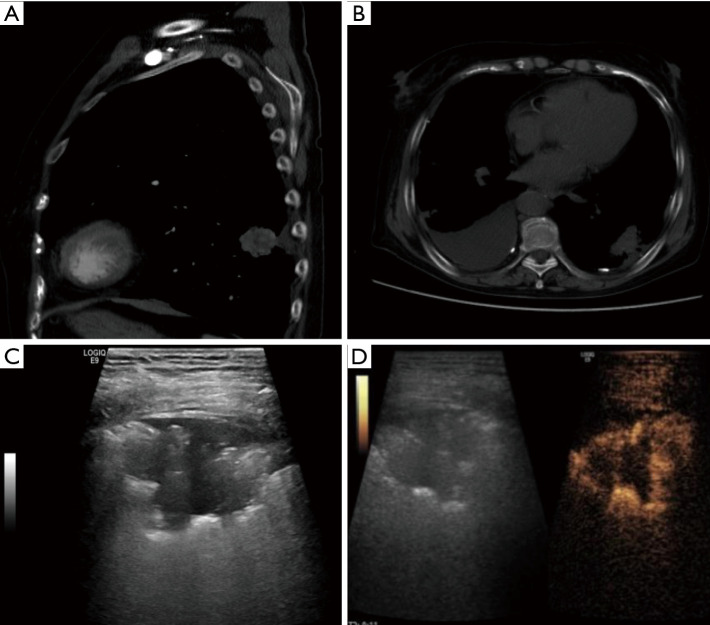
Ninety-two peripheral lung lesions in 92 patients, detected via computed tomography (CT) and also visible on ultrasound, were retrospectively analyzed. All patients underwent percutaneous peripheral lung lesion needle biopsy under traditional ultrasound or contrast enhanced ultrasound (CEUS) guidance paying attention to avoiding necrotic areas and large blood vessels. All the specimens were examined histopathologically. Preprocedure all 92 lesions were performed by traditional ultrasonography to evaluate the size, the echogenecity, liquefaction areas and blood flow on color Doppler imaging, some of which were performed by CEUS for evaluating non-enhanced necrosis areas, contrast agent arrival time (AT) and characteristics of blood perfusion.
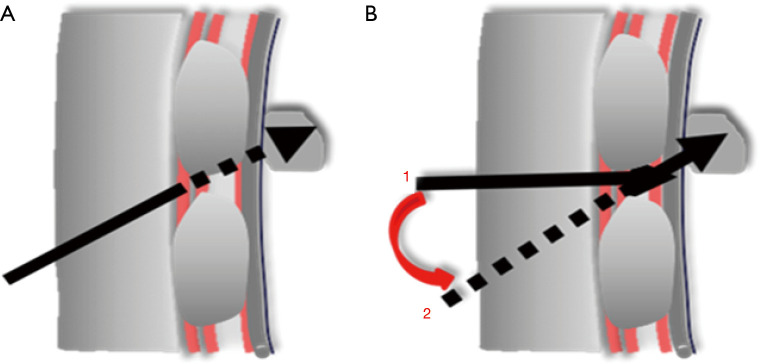
The histopathologic results of all 92 lesions were as follows: 67 malignant tumors (including 28 adenocarcinomas, 19 squamous cell carcinomas, 6 bronchoalveolar carcinomas, 5 small cell carcinomas, 5 metastatic cancers, 3 poorly differentiated cancers and 1 malignant mesothelioma), 20 benign lesions (including 9 pneumonia, 6 inflammatory pseudotumors and 5 tuberculomas), 5 undetermined lesions. Of 52 lesions by CEUS guidance, 7 lesions showed enhancement in the pulmonary arterial-phase (including 6 pneumonia and 1 malignant tumors), 45 lesions showed enhancement in the bronchial artery phase (including 37 malignant tumors, 3 inflammatory pseudotumors, 4 tuberculomas and 1 undetermined lesion). According to needle insertion angle along linear path, a total of 92 lesions were divided into two groups, 49 lesions at an angle of 70°-80° needle insertion and 43 lesions at an angle of 80°-90° needle insertion. In the study, linear and non-linear two puncture paths were used, we first tried to puncture along linear path in all lesions, if an attempt to insert into the lesions failed due to be blocked by the ribs and then changed to puncture along non-linear path instead. The success rate of biopsy procedure along linear puncture was significantly higher at an angle of 80°-90°group (93.0% 20.4%, P<0.01), and the adoption rate of non-linear path biopsy for solving the puncture needle blocked by the ribs was significantly higher at angle of 70°-80°group (79.6% 7.0%, P<0.01). Of 52 lesions by CEUS guidance, 27 (51.9%) showed non enhanced necrosis areas on CEUS, only 5 showed liquefaction necrosis areas on gray-scale ultrasound. Of 40 lesions by traditional ultrasound guidance, 4 showed necrosis areas on gray-scale ultrasound. There were no significant differences in lesion size, the average number of biopsy attempts and complication rates between CEUS guidance group and traditional ultrasound guidance group (P>0.05), the pathological confirmation rate in CEUS guidance group was higher than that in traditional ultrasound guidance group, but without significant difference (98.1% 90.0%, P>0.05). Of all 92 cases, 3 cases (3.3%) had mild pneumothorax and 4 cases (4.3%) had hemoptysis.
In ultrasound-guided needle biopsy for peripheral lung lesions, using a combination of linear and non-linear puncture techniques and keeping away from necrotic areas and large blood vessels, may help to increase the success rate and reduce the incidence of complications further.
探讨超声引导下经皮穿刺针吸活检术用于周围型肺病变的穿刺技巧及并发症预防。
回顾性分析92例患者的92个经计算机断层扫描(CT)发现且超声可见的周围型肺病变。所有患者均在传统超声或超声造影(CEUS)引导下进行经皮周围型肺病变穿刺针吸活检,注意避开坏死区域和大血管。所有标本均进行组织病理学检查。术前对所有92个病变均行传统超声检查,以评估其大小、回声、液化区及彩色多普勒血流情况,部分病变行CEUS检查以评估无增强坏死区、造影剂到达时间(AT)及血流灌注特征。
92个病变的组织病理学结果如下:恶性肿瘤67个(包括腺癌28个、鳞癌19个、细支气管肺泡癌6个、小细胞癌5个、转移癌5个、低分化癌3个及恶性间皮瘤1个),良性病变20个(包括肺炎9个、炎性假瘤6个及结核瘤5个),未确定病变5个。在CEUS引导下的52个病变中,7个病变在肺动脉期有增强(包括肺炎6个、恶性肿瘤1个),45个病变在支气管动脉期有增强(包括恶性肿瘤37个、炎性假瘤3个、结核瘤4个及未确定病变1个)。根据沿直线路径的进针角度,将92个病变分为两组,进针角度为70° - 80°的病变49个,进针角度为80° - 90°的病变43个。本研究采用直线和非直线两种穿刺路径,所有病变均先尝试沿直线路径穿刺,若因肋骨阻挡穿刺针无法插入病变,则改为沿非直线路径穿刺。直线穿刺活检成功率在进针角度为80° - 90°组显著更高(93.0% 20.4%,P<0.01),非直线路径活检用于解决肋骨阻挡穿刺针问题的采用率在进针角度为70° - 80°组显著更高(79.6% 7.0%,P<0.01)。在CEUS引导下的52个病变中,27个(51.9%)在CEUS上显示无增强坏死区,仅5个在灰阶超声上显示液化坏死区。在传统超声引导下的40个病变中,4个在灰阶超声上显示坏死区。CEUS引导组与传统超声引导组在病变大小、平均活检次数及并发症发生率方面差异无统计学意义(P>0.05),CEUS引导组的病理确诊率高于传统超声引导组,但差异无统计学意义(98.1% 90.0%,P>0.05)。92例患者中,3例(3.3%)发生轻度气胸,4例(4.3%)出现咯血。
在超声引导下对周围型肺病变进行穿刺活检时,采用直线和非直线穿刺技术相结合并避开坏死区域和大血管,可能有助于进一步提高成功率并降低并发症发生率。