Sang Ling, Nong Lingbo, Zheng Yongxin, Xu Yonghao, Chen Sibei, Zhang Yu, Huang Yongbo, Liu Xiaoqing, Li Yimin
State Key Laboratory of Respiratory Disease, National Clinical Research Center for Respiratory Disease, Guangzhou Institute of Respiratory Health, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou, China.
J Thorac Dis. 2020 Jul;12(7):3725-3736. doi: 10.21037/jtd-20-1050.
Adequate respiratory support can improve clinical outcomes in patients who are ready for weaning from a ventilator. We aimed to investigate the efficacy of respiratory methods in adults undergoing planned extubation using a Bayesian network meta-analysis.
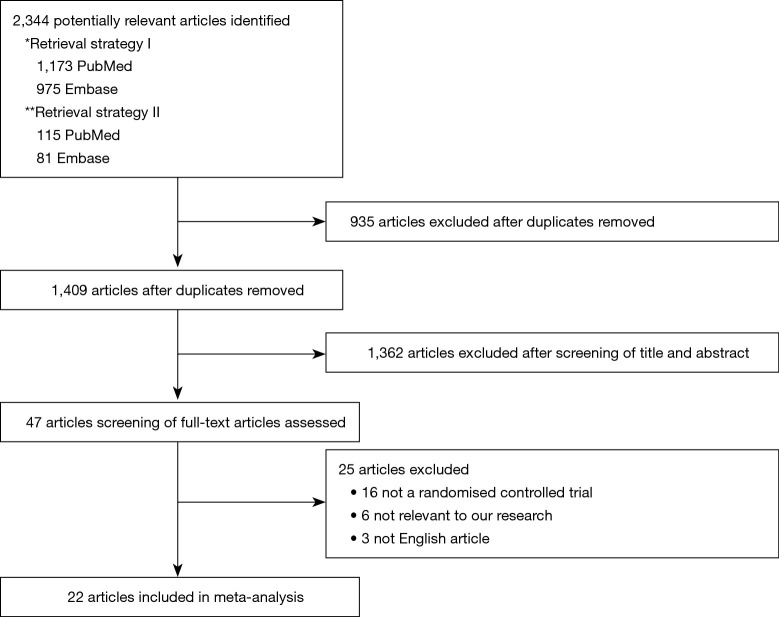
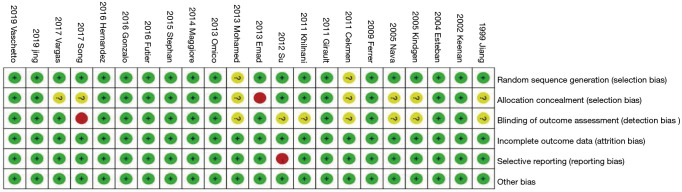
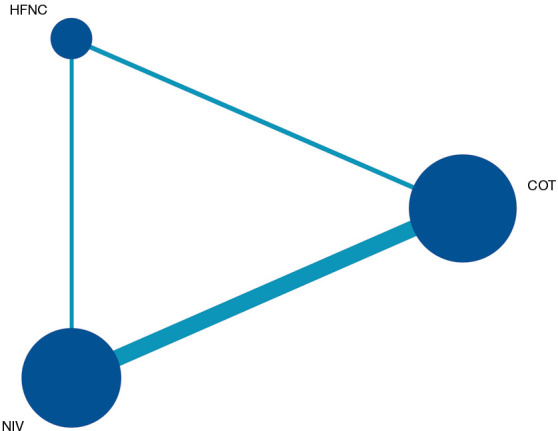
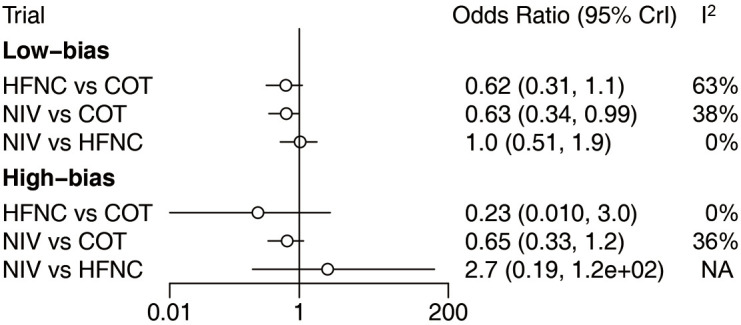
We searched PubMed, Embase, and ClinicalTrials.gov for unpublished and ongoing trials up to November 2019 for randomized controlled trials (RCTs) published in English that compared conventional oxygen therapy (COT), a high-flow nasal cannula (HFNC), and noninvasive ventilation (NIV) for post-extubation respiratory support. Screening of citations, study selection, data extraction, and assessment of risk were performed independently by two authors. The primary outcome was the reintubation rate.
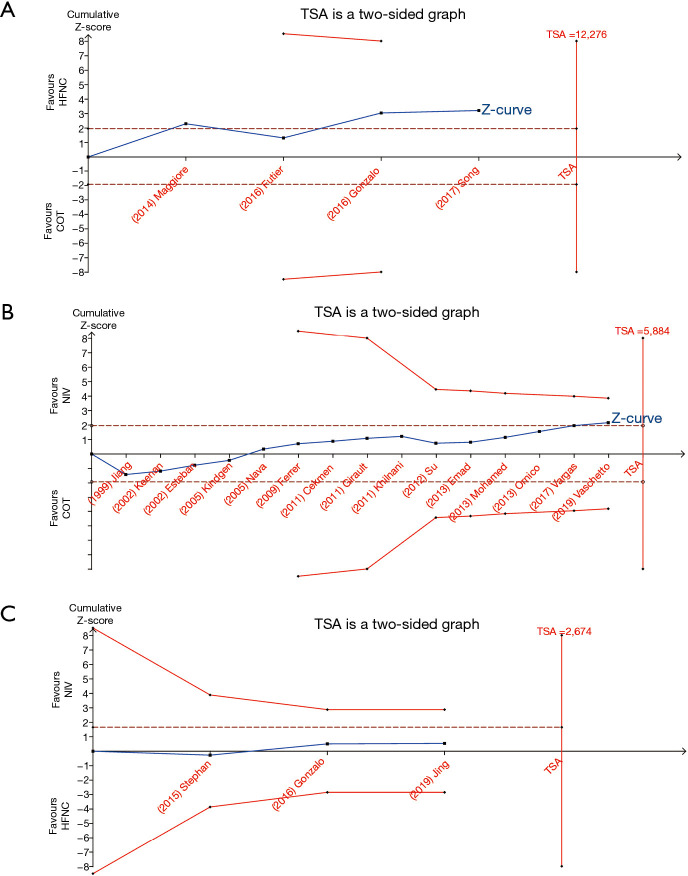
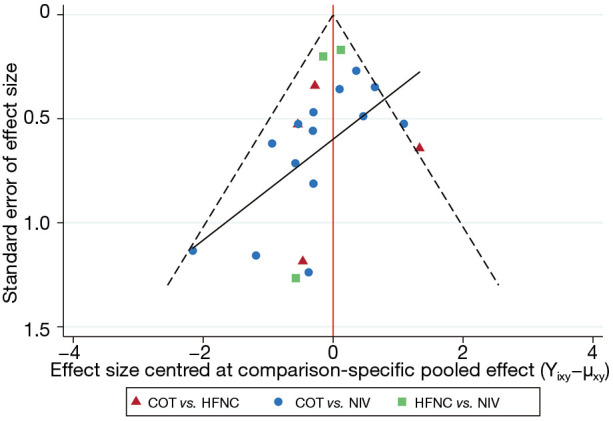
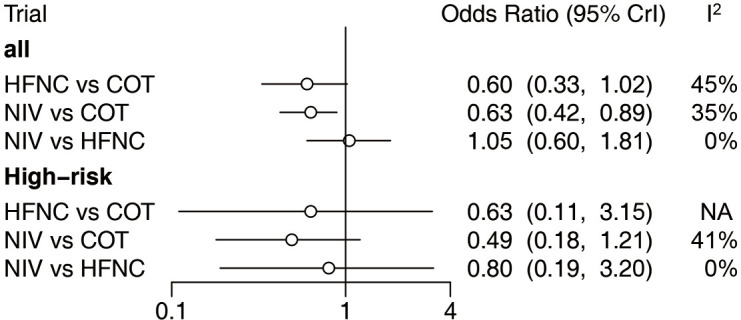
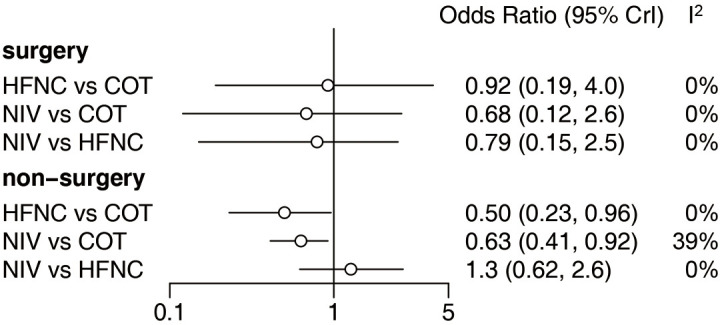
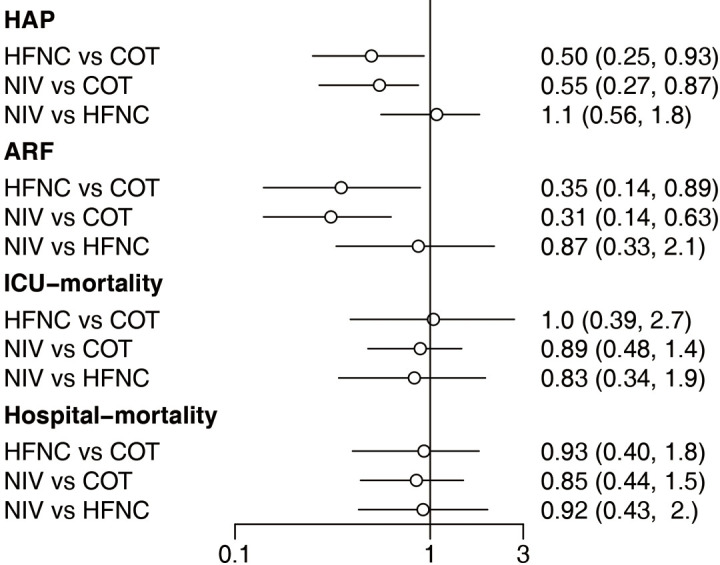
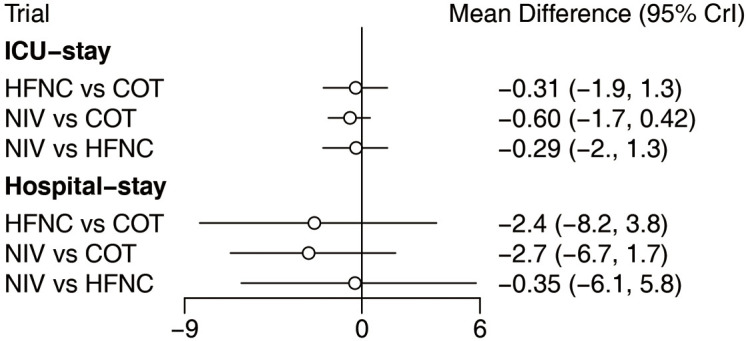
Twenty-two studies (4,218 patients) were included in our meta-analysis. Extubated patients supported with NIV had a significantly lower incidence of reintubation than those supported with COT [odds ratio (OR): 0.63, 95% confidence interval (CI): 0.42, 0.89]. However, there was no significant difference in the reintubation rate between the HFNC and NIV, and HFNC and COT groups (OR: 1.05, 95% CI: 0.60, 1.81; OR: 0.60, 95% CI: 0.33, 1.02, respectively). HFNC and NIV reduced the incidence of hospital-acquired pneumonia (HAP) (OR: 0.50, 95% CI: 0.25, 0.93; OR: 0.55, 95% CI: 0.27, 0.87, respectively) and post-extubation acute respiratory failure (ARF) (OR: 0.35, 95% CI: 0.14, 0.89; OR: 0.31, 95% CI: 0.14, 0.63, respectively) compared with COT. There was no significant difference in a decreased incidence of HAP (OR: 1.1, 95% CI: 0.56, 1.8) or post-extubation ARF (OR: 0.87, 95% CI: 0.33, 2.1) between NIV and HFNC. There were also no significant differences in improvements in other clinical outcomes, including intensive care unit (ICU) and hospital mortality and the length of stay (LOS) between NIV and HFNC.
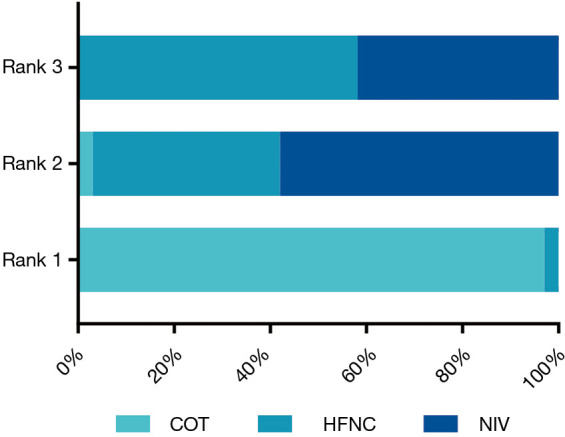
NIV reduces the reintubation rate in adult patients undergoing planned extubation compared with COT and HFNC.
充分的呼吸支持可改善准备撤机患者的临床结局。我们旨在通过贝叶斯网络荟萃分析研究呼吸方法对计划拔管的成年患者的疗效。
我们检索了PubMed、Embase和ClinicalTrials.gov,以查找截至2019年11月未发表和正在进行的试验,纳入以英文发表的比较传统氧疗(COT)、高流量鼻导管(HFNC)和无创通气(NIV)用于拔管后呼吸支持的随机对照试验(RCT)。两名作者独立进行文献筛选、研究选择、数据提取和风险评估。主要结局是再插管率。
我们的荟萃分析纳入了22项研究(4218例患者)。接受NIV支持的拔管患者再插管发生率显著低于接受COT支持的患者[比值比(OR):0.63,95%置信区间(CI):0.42,0.89]。然而,HFNC与NIV组以及HFNC与COT组之间的再插管率无显著差异(OR分别为:1.05,95%CI:0.60,1.81;OR:0.60,95%CI:0.33,1.02)。与COT相比,HFNC和NIV降低了医院获得性肺炎(HAP)的发生率(OR分别为:0.50,95%CI:0.25,0.93;OR:0.55,95%CI:0.27,0.87)以及拔管后急性呼吸衰竭(ARF)的发生率(OR分别为:0.35,95%CI:0.14,0.89;OR:0.31,95%CI:0.14,0.63)。NIV与HFNC之间在降低HAP发生率(OR:1.1,95%CI:0.56,1.8)或拔管后ARF发生率(OR:0.87,95%CI:0.33,2.1)方面无显著差异。在其他临床结局改善方面,包括重症监护病房(ICU)和医院死亡率以及住院时间(LOS),NIV与HFNC之间也无显著差异。
与COT和HFNC相比,NIV可降低计划拔管成年患者的再插管率。