The First Clinical Medical College, Lanzhou University, Lanzhou City, Gansu Province, People's Republic of China.
Int J Chron Obstruct Pulmon Dis. 2022 Aug 30;17:1987-1999. doi: 10.2147/COPD.S375107. eCollection 2022.
To evaluate the clinical efficacy of high-flow nasal oxygen therapy (HFNC) and non-invasive ventilation (NIV) in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) after extubation.
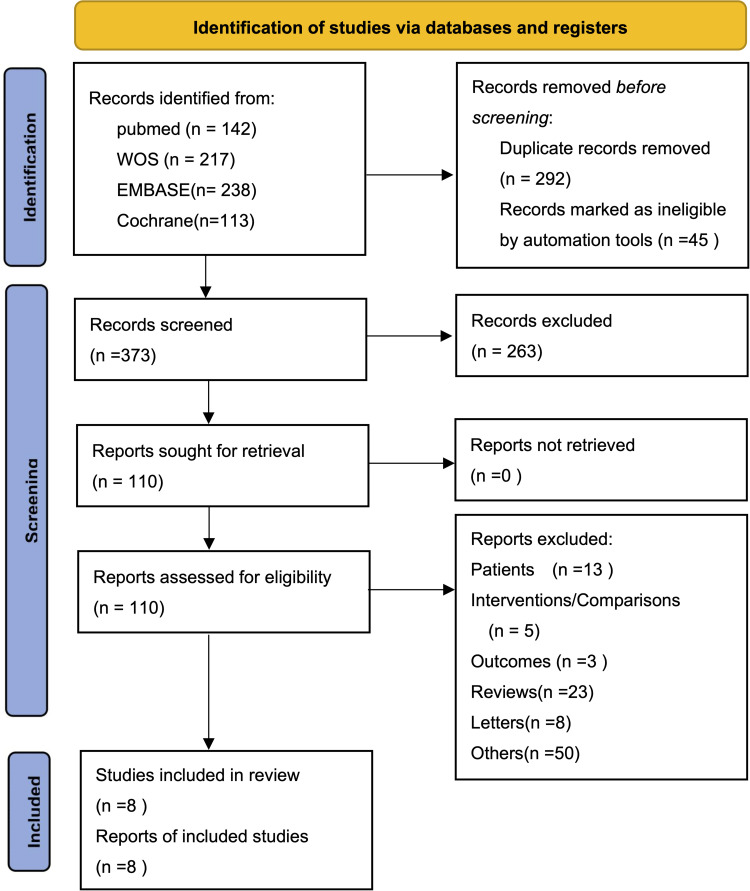
This systematic review and meta-analysis was conducted following the Preferred Reporting Items for Systematic Review and Meta-analyses (PRISMA) statements. The primary outcome measures analyzed included: reintubation rate, mortality, complication rate, and ICU length of stay.
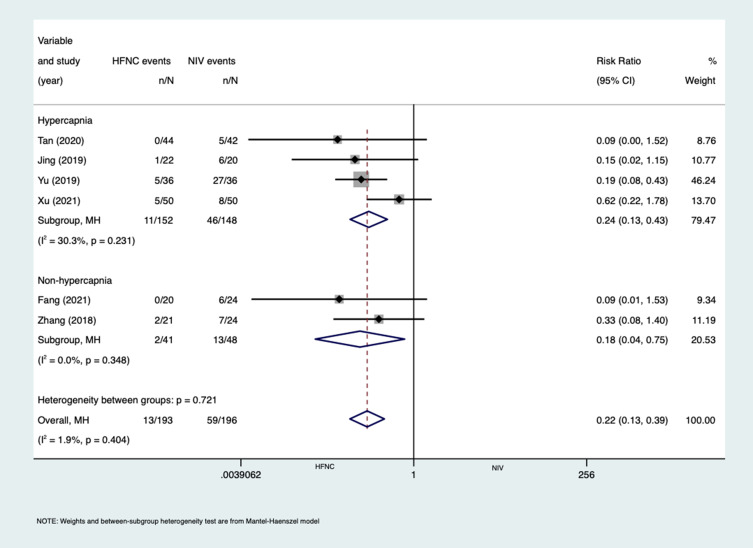
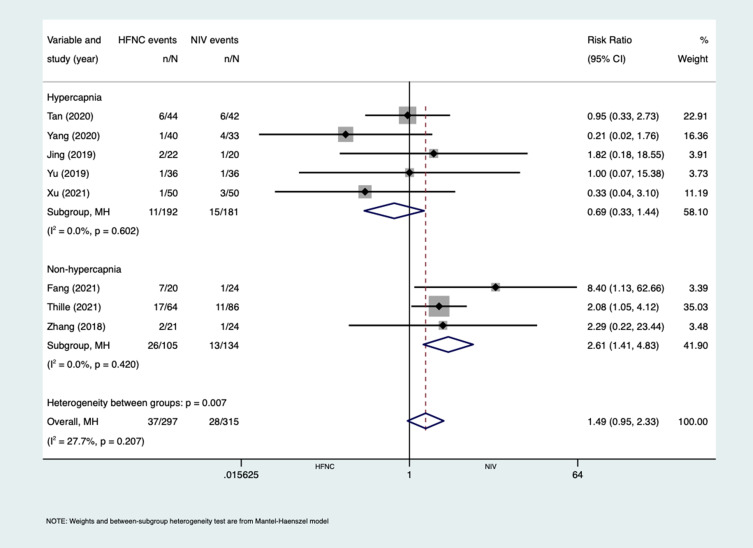
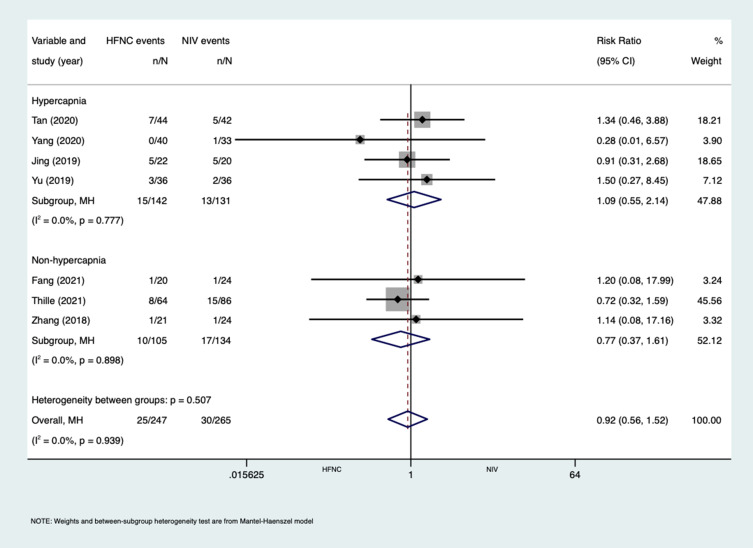
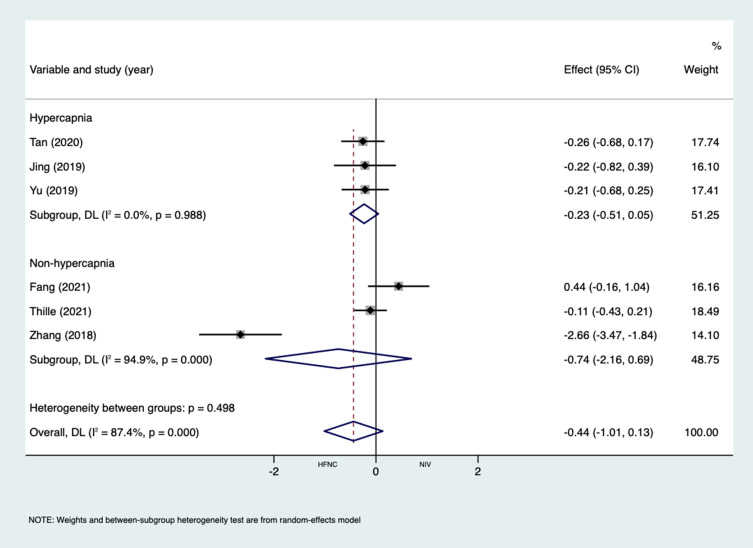
Eight studies were included, with a total of 612 subjects, including 297 in the HFNC group and 315 in the NIV group. The effect of HFNC and NIV on the reintubation rate of AECOPD patients after extubation, RR (1.49 [95% CI,0.95 to 2.33], P = 0.082). Subgroup analysis with or without hypercapnia according to the included AECOPD population, with hypercapnia, RR (0.69 [95% CI,0.33 to 1.44], P=0.317), without hypercapnia, RR (2.61 [95% CI,1.41 to 4.83], P=0.002). Mortality, RR (0.92 [95% CI,0.56 to 1.52], P = 0.752). ICU length of stay, MD (-0.44 [95% CI,-1.01 to 0.13], P = 0.132). Complication rate, RR (0.22 [95% CI,0.13 to 0.39], P = 0.000). After subgroup analysis, the reintubation rate of HFNC and NIV has no statistical difference in patients with hypercapnia, but NIV can significantly reduce the reintubation rate in patients without hypercapnia. In the outcome measures of complication rate, HFNC significantly reduced complication rate compared with NIV. In mortality and ICU length of stay, analysis results showed that HFNC and NIV were not statistically different.
According to the available evidence, the application of HFNC can be used as an alternative treatment for NIV after extubation in AECOPD patients with hypercapnia, but in the patients without hypercapnia, HFNC is less effective than NIV.
评估高流量鼻氧疗(HFNC)和无创通气(NIV)在慢性阻塞性肺疾病急性加重(AECOPD)患者拔管后的临床疗效。
本系统评价和荟萃分析遵循系统评价和荟萃分析的首选报告项目(PRISMA)声明。主要结局指标包括:再插管率、死亡率、并发症发生率和 ICU 住院时间。
纳入 8 项研究,共 612 例患者,其中 HFNC 组 297 例,NIV 组 315 例。HFNC 和 NIV 对拔管后 AECOPD 患者再插管率的影响,RR(1.49[95%CI,0.95 至 2.33],P=0.082)。根据纳入的 AECOPD 人群中是否伴有高碳酸血症进行亚组分析,伴有高碳酸血症,RR(0.69[95%CI,0.33 至 1.44],P=0.317),不伴有高碳酸血症,RR(2.61[95%CI,1.41 至 4.83],P=0.002)。死亡率,RR(0.92[95%CI,0.56 至 1.52],P=0.752)。ICU 住院时间,MD(-0.44[95%CI,-1.01 至 0.13],P=0.132)。并发症发生率,RR(0.22[95%CI,0.13 至 0.39],P=0.000)。亚组分析后,HFNC 和 NIV 在伴有高碳酸血症的患者中再插管率无统计学差异,但 NIV 可显著降低无高碳酸血症患者的再插管率。在并发症发生率的结局指标中,HFNC 与 NIV 相比显著降低了并发症发生率。在死亡率和 ICU 住院时间方面,分析结果表明 HFNC 和 NIV 无统计学差异。
根据现有证据,HFNC 可作为伴有高碳酸血症的 AECOPD 患者拔管后 NIV 的替代治疗方法,但在不伴有高碳酸血症的患者中,HFNC 不如 NIV 有效。